

NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-.

ABSTRACT
Thyroid cancer accounts for only 0.4% of all cancer deaths, with an incidence of 11 cases and about 0.5-0.6 deaths per 100,000 population in the United States each year,according to the November 2011 SEER report (http://seer.cancer.gov/statfacts/html/thyro.html). Its clinical importance, by contrast, is out of all proportion to its incidence, because cancers of the thyroid must be differentiated from the much more frequent benign adenomas and multinodular goiters. The latter, depending on the criteria employed, occur in up to 4% of the population, and thyroid nodules may be present in 20% or more of adults subjected to routine thyroid echography. The differential diagnosis of thyroid nodules is now easily accomplished by fine needle aspiration cytology in 60-90% of the cases, allowing a significant reduction in the number of thyroid surgeries performed for thyroid nodules. This chapter is concerned with the clinical and pathological description of benign and malignant thyroid nodules and with the diagnostic and therapeutic approach to them. What will be said applies also to nodules found within a multinodular goiter, although as a separate entity this disease is discussed in Chapter 17.
INTRODUCTION
Numerous classifications of thyroid tumors have been proposed. The one we currently follow groups the lesions on the basis of histologic findings (Table 18-1). The frequently encountered papillary tumors can be subdivided into the small proportion that have only papillary histologic characteristics and the larger group having, in addition, follicular elements. There is no agreement that these groups differ functionally, and current terminology treats them as one.
DEFINITION
The thyroid adenoma is a benign neoplastic growth contained within a capsule. The term adenoma and nodule are often used interchangeably in the literature. This practice is imprecise because adenoma implies a specific benign new tissue growth with a glandlike cellular structure, whereas a nodule could as well be a cyst, carcinoma, lobule of normal tissue, or other focal lesion different from the normal gland. In the following section, the term nodule appears frequently when there is need for a nonspecific term.
Table 18-1Neoplasms of the Thyroid (Adapted, and Revised, from WHO Classification)(1)
I. Adenomas (Fig. 18-1, below)
A. Follicular
1. Colloid variant
2. Embryonal
3. Fetal
4. Hurthle cell variant
B. Papillary (probably malignant)
C. TeratomaII. Malignant Tumors
A. Differentiated
1. Papillary adenocarcinoma
a. Pure papillary adenocarcinoma
b.Mixed papillary and follicular carcinoma
(variants including tall cell, follicular, oxyphyl, solid)
2. Follicular adenocarcinomas (variants: "malignant
adenoma", Hurthle cell carcinoma or oxyphil
carcinoma, clear-cell carcinoma, insular carcinoma)
B. Medullary carcinoma- (not a tumor of follicular cells)
C. Undifferentiated
1. Small cell (to be differentiated from lymphoma)
2. Giant cell
3. Carcinosarcoma
D. Miscellaneous
1. Lymphoma, sarcoma
2. Squamous cell epidermoid carcinoma
3. Fibrosarcoma
4. Mucoepithelial carcinoma
5. Metastatic tumor
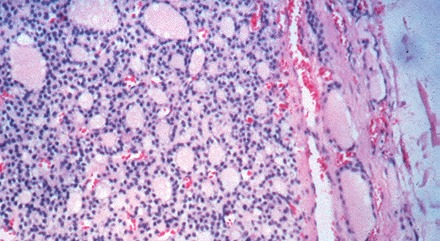
Figure 18-1A) Follicular and microfollicular adenoma. The nodule shows microfollicles, is sharply circumscribed by a delicate even fibrous capsule, and there is no invasion of the capsule or blood vessels by the tumor.
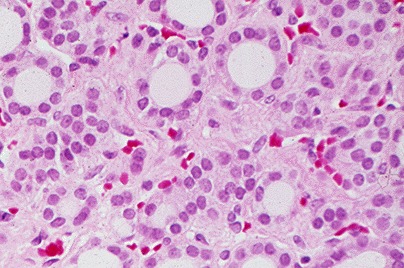
Figure 18-1B) The central area of a microfollicular adenoma displays regular nuclei and some interfollicular edema.
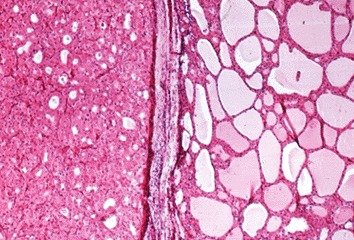
Figure 18-1C) Hurthle (oxyphile) cell tumor, lower half of photomicrograph, with well circumscribed margin established by an intact delicate fibrous capsule. This is a Hurthle cell tumor of low malignant potential (an adenoma).
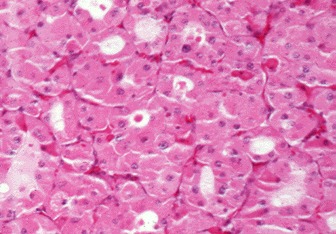
Figure 18-1D) High power view of a Hurthle cell tumor made up of microfollicles lined by large acidophilic cells, the cytoplasm of which is granular and filled with mitochondria.
PATHOLOGY OF NODULES
Thyroid nodules are not expression of a single disease but are the clinical manifestation of a wide range of different diseases. Non-neoplastic nodules are the result of glandular hyperplasia arising spontaneously or following partial thyroidectomy; rarely, thyroid hemiagenesia may present as hyperplasia of the existing lobe, mimicking a thyroid nodule. Non-neoplastic thyroid diseases, such as Hashimoto’s thyroiditis or subacute thyroiditis may appear as thyroid lumps which are not true nodules but just the expression of the underlying thyroid disease.
Benign neoplastic nodules are divided into embryonal, fetal, follicular, Hurthle, and possibly papillary adenomas on the basis of their characteristic pattern 12. Examples appear in Figure 18-1 (above). The adenomas usually exhibit a uniform orderly architecture and few mitoses, and show no lymphatic or blood vessel invasion. They are characteristically enveloped by a discrete fibrous capsule or a thin zone of compressed surrounding thyroid tissue. All types of nodules may become partially cystic, presumably through necrosis of a portion of the growth. Cyst formation is very common in colloid nodules.
Whether papillary adenoma is a real entity is debatable; most observers believe that all papillary tumors should be considered as carcinomas. Others consider that some papillary tumors are benign adenomas. It is our impression that papillary tumors are best thought of as carcinomatous, although the degree of invasive potential may be very slight in some instances. The same confusion extends to Hurthle cell adenomas. Many pathologists consider all of these tumors as low-grade carcinomas in view of their frequent late recurrences. For this reason, the nondefinitive term Hurthle cell tumor is commonly used. Pathologists usually grade them on the probability of being malignant, based on factors such as invasion of the thyroid tumor capsule or blood vessels, without differentiation into benign and malignant. Hurthle cell tumors are found on electron microscopy to be packed with mitochondria, which accounts for their special eosinophilic staining quality.
Nearly half of all single nodules have on gross inspection a gelatinous appearance, are composed of large colloid-filled follicles, and are not completely surrounded by a well-defined fibrous capsule. These nodules are listed as colloid variants of follicular adenomas in our classification. Many pathologists report these as colloid nodules, and suggest that each is a focal process perhaps related to multinodular goiter rather than a true adenoma. These tumors are usually not surrounded by a capsule of compressed normal tissue, and often show degeneration of parenchyma, hemosiderosis, and colloid phagocytosis (Fig. 18-2). Recent studies indicate that most adenomas, as well as carcinomas, are truly clonal -- derived from one cell -- whereas colloid nodules, at least in multinodular goiters, tend to be polyclonal (2).

Figure 18-2A) "Colloid nodules" display macrofollicles lined by flattened thyroid epithelial cells. The nodules are circumscribed and do not have a fibrous capsule.
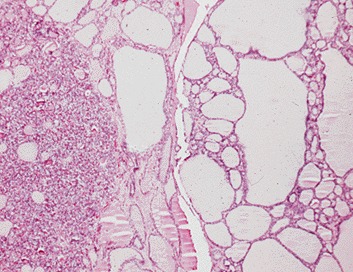
Figure 18-2B) Possible evolution of a "colloid nodule". An area of nodular hyperplasia on left, and a "developing" colloid nodule on right, with macrofollicles and some remaining focal hyperplasia.
Figure 18-3. Fine needle aspiration cytology specimens.
CAUSE OF NODULES
Thyroid adenomas are monoclonal "new growths" that are formed in response to the same sort of stimuli as are carcinomas. Heredity does not appear to play a major role in their appearance. One clue to their origin is that they are four times more frequent in women than in men, although no definitive relation of estrogen to cell growth has been demonstrated. Thyroid radiation, chronic TSH stimulation, and oncogenes believed to be related to the origin of these lesions are discussed below in the section on thyroid cancer. Of specific interest in relation to benign nodules is the remarkable observation by Vassart and colleagues that activating mutations of the TSH receptor are the specific cause of most autonomously functioning thyroid nodules (3) including those found in the context of a mulitnodular goiter (4). Please see the discussion on causation under "Carcinoma".
COURSE AND SYMPTOMS OF NODULES
Thyroid adenomas grow slowly and may remain dormant for years. This is presumably related to the fact that adult thyroid cells normally divide once in eight years. (5) Pregnancy tends to make nodules increase in size, and to cause development of new nodules. An adenoma may first come to attention because the patient accidentally finds a lump in the neck or because a physician discovers it upon routine examination. Rarely, symptoms such as dysphagia, dysphonia, or stridor may develop, but it is unusual for these tumors to attain sufficient size to cause significant symptoms in the neck. Typically, they are entirely asymptomatic. Occasionally there is bleeding into the tumor, causing a sudden increase in size and local pain and tenderness. After bleeding into an adenoma, transient symptoms of thyrotoxicosis may appear with elevated serum T4 levels, and suppression of thyroidal RAIU. Spontaneous regression of adenomas can occur.
M.G., 47-Year-Old Woman: Hemorrhage into a Nodule
When the patient was first examined, enlargement of the thyroid had been known for at least 6 years. A scan showed a cold nodule in the left lobe. The patient was thought to have a thyroid nodule and to be euthyroid. There was on exam a normal right thyroid lobe, and a 4 x 5 cm soft mass occupying the position of the left lobe. The impression at this time was that she had an adenoma that might be cystic. Antithyroid antibodies were not detectable.
The patient was examined by several observers who palpated the thyroid. One-half hour after leaving the clinic, the patient's neck gradually began to enlarge, and she developed pain in the area of the thyroid and a rasping hoarseness. She had no difficulty in swallowing or breathing. The pain was significant enough to keep her awake that night, and she returned to the hospital the next day. The patient was very anxious, and there was a 10 x 12-cm tender fluctuant swelling occupying the area of the thyroid. Inspiratory stridor was present, and there were a few rhonchi in the lungs.
During the subsequent 3 days the pain in the neck gradually diminished, but the size of the mass remained more or less the same. Chest x-ray films revealed marked deviation of the trachea to the right. Operation was elected. A greatly enlarged left lobe of the thyroid was found, with hemorrhage into an adenoma. The encapsulated mass measured 6.5 x 5.5 cm and was smooth and cystic. There was a large multiloculated hematoma and considerable necrotic tissue. A left lobectomy was performed. Microscopic examination showed a microfollicular thyroid adenoma with recent hemorrhage and necrosis. The postoperative course was unremarkable. The patient remained well after surgery without further difficulty.
Usually hemorrhage occurs without known provocation, but occasionally is seen after trauma to the neck. In this instance, palpation may have been sufficient to induce bleeding.
Does an adenoma ever develop into a carcinoma? At the practical level, thyroid adenomas appear to be benign from the start and most thyroid carcinomas are likewise malignant from their inception, and do not appear on pathological examination to originate in an adenoma. Perhaps this has to do with the specific discrete mutational event causing their development. However, in animals chronically given 131-I and antithyroid drugs, a gradual progression of types of lesions from adenomas to carcinomas is seen. Pathologic examination occasionally gives evidence for conversion of an adenoma to a carcinoma. Transformation of hyperplastic thyroid tissue into invasive cancer occurs in occasional patients with congenital goitrous hypothyroidism, and occasionally cancers are seen inside an adenoma or in a gland that was known to have harbored a nodule for many years. Occasionally a patient develops metastatic cancer years after resection of an embryonal or Hurthle cell adenoma. Rearrangement of the RET gene, the genetic abnormality responsible for a subset of papillary thyroid carcinoma, is frequently found in microcarcinoma, suggesting that this lesion is malignant from the beginning without the need for accumulating several genetic lesions (6). Furthermore, no case of RET/PTC positive anaplastic cancer has been found up to now, again suggesting that there is no transition from papillary, at least RET/PTC positive, carcinoma to anaplastic cancer (6). All of these points suggest that transformation of an adenoma into a carcinoma occurs occasionally, but it appears to be an unusual sequence of events.
HOT NODULES
About 10% of thyroid follicular adenomas are functional enough (are "hot" on scan) to produce overt thyrotoxicosis or subclinical hyperthyroidism (suppressed TSH being the only abnormality) and account for perhaps 2% of all thyrotoxic patients. Another 10% may be borderline in function and are classified as warm or "hot" (or hyperfunctioning, in comparison to the remainder of the thyroid gland) on isotopic scans. Although hyperfunctioning nodules may remain unchanged for years, some gradually develop into toxic nodules, especially if their diameter exceeds 3 cm (7). Others undergo spontaneous necrosis with a return of function in the formerly suppressed normal gland. Patients with functioning autonomous nodules may be overtly thyrotoxic; more commonly, however, the nodule functions enough to suppress the remainder of the gland, but not enough to produce clinical hyperthyroidism (8). In such patients, T3 levels may be slightly elevated, serum TSH below normal, and the pituitary response to TRH is typically suppressed (9). If the nodule is resected, the gland resumes normal function, and serum TSH and the TRH response is normalized (see also Chapter 13).
In certain areas such as Switzerland, up to one-third of all thyrotoxic patients have hyperfunctioning adenomas (10), largely in multinodular glands. Perhaps this situation is generally true in endemic goiter areas.
Activating TSH receptor mutations have been found by Vassart and co-workers (11) to be the cause of most hyperfunctional nodules, and are now known to be common in "hot" nodules in patients with multi-nodular goiter.. These mutations generally involve the extracellular loops of the transmembrane domain and the transmembrane segments, and are proven to induce hyperfunction by transfection studies. Mutations of the stimulatory GTP binding protein subunit are also present in some patients with hyperfunctioning thyroid adenomas (12).
METABOLIC FUNCTION OF NODULES
The biochemical defect responsible for diminished iodine metabolism in the "cold" (i.e., inactive) nodule can result from deletion of specific metabolic processes required for hormone synthesis. Slices of cold nodules incubated in vitro were unable to accumulate iodide against a concentration gradient, although peroxidase and iodide organification activities were present (13). This finding was consistent with a specific defect of the iodide transport process. Others have also observed this phenomenon and have shown that TSH can bind to the membranes of the cells and activate adenyl cyclase as usual, but that subsequent metabolic steps are not induced (14). Activity of the sodium-potassium-activated ATPase, thought to be related to iodide transport, is intact, and ATP levels are normal, even though iodide transport is inoperative. Other nodules appear to be cold because they lack peroxidase (15). These nodules can be "hot" when scanned with 99mTcO4 due to active transport of the isotope, but relatively cold on scanning at 24 hours after 131-I is given, since iodide binding is poor (16). The adenyl cyclase system in the plasma membrane of some hyperfunctioning nodules has been found to be hyper-responsive to TSH in some studies (17) but not in others (18). As noted above, most hyperfunctional nodules are associated with- presumably caused by- activating mutations of the TSH receptor. All of the foregoing reports suggest that adenoma formation is associated with mutational events that cause loss or dysfunction of normal metabolic activities The recent cloning of the sodium/iodide synporter gene (NIS) (19) has allowed the study of its expression in thyroid nodules. NIS expression is increased, with respect to normal thyroid tissue, in hyperfunctioning nodules and low or absent in cold nodules both benign and malignant (20).
CLINICAL EVALUATION AND MANAGEMENT OF NODULES
Table 18-2 Differential Diagnosis of the Thyroid Nodule
Adenoma
Cyst
Carcinoma
Multinodular goiter
Hashimoto's thyroiditis
Subacute thyroiditis
Effect of prior operation or 131I therapy
Thyroid hemiagenesis
Metastasis
Parathyroid cyst or adenoma
Thyroglossal cyst
Nonthyroidal lesions
Inflammatory or neoplastic nodes
Cystic hygroma
Aneurysm
Bronchocele
Laryngocele
HISTORY OF NODULES
Conditions to be considered in the differential diagnosis are listed in Table 18-2. They include adenoma, cyst, multinodular goiter, a prominent area of thyroiditis, an irregular regrowth of tissue if surgery has been performed, thyroid hemiagenesis, and of course, thyroid cancer. Hashimoto's thyroiditis offten presents with a lumpy gland on physical exam, and a nodular or pseudo-nodular appearance on ultrasound is frequent. In some patients Hurthle cell rich nodular areas develop, and of course some patients have coexistent but (presumably) etiologically distinct adenomas or cancers.
Factors that must be considered in reaching a decision for management include the history of the lesion, age, sex, and family history of the patient, physical characteristics of the gland, local symptoms, and laboratory evaluation. The age of the patient is an important consideration since the ratio of malignant to benign nodules is higher in youth and lower in older age. Male sex carries a similar importance (21). Nodules are less frequent in men, and a greater proportion are malignant.
Rarely, the family history may be helpful in the decision regarding surgery. Patients with the hereditable multiple endocrine neoplasia syndrome (MEN), type I, may have thyroid adenomas, parathyroid adenomas, islet cell tumors, and adrenal tumors, whereas patients with MEN types II and III, have pheochromocytomas, medullary thyroid carcinomas, hyperparathyroidism, and mucosal neuromas (22-24) (vi). Further, we have observed that 6% of our patients with thyroid carcinoma have a history of malignant thyroid neoplasm in other family members, and familial medullary cancer (without MEN) is well known. Familial thyroid tumors occur in Cowden's disease, Gardner's syndrome, and familial polyposis coli (vi.)
A most important piece of information regarding a nodule is a history of prior neck irradiation. Any irradiation above 50 rads (50 cGrays) to the thyroid during childhood should be viewed with concern. Exposure to 100-700 rads during the first 3 or 4 years of life has been associated with a 1-7% incidence of thyroid cancer occurring 10-30 years later (25-30). Radiation exposure during adolescence or early adulthood for acne or for other reasons has also been identified as a cause of this disease. Although this association was known by 1950, patients were still being seen with radiation-related tumors who received x-ray treatment as late as 1959. Radiation therapy for other benign or malignant lesions in the neck is still in use in selected patients; such exposure will thus continue to be a relevant part of the history. Because of the high prevalence (20-40%) of carcinoma in nodules resected from irradiated glands, the finding of one or more clear-cut nodules in a radiated gland, or a cold area on scan, must be viewed with alarm and requires consideration for removal, as indicated below. In this case, multiple nodules do not indicate that the lesions are benign. In contrast, prior exposure to internal radiation from 131-I for diagnostic or therapeutic purposes has not to date been associated with an increased risk of developing thyroid carcinoma.
The history of the neck lump itself is important. Recent onset, growth, hoarseness, pain, nodes in the supraclavicular fossae, symptoms of brachial plexus irritation, and local tenderness all suggest malignancy, but of course do not prove it. The usual cause of sudden swelling and tenderness in a nodule is hemorrhage into a benign lesion. Although the presence of a nodule for many years suggests a benign process, some cancers grow slowly. In our series, the average time from recognition of a nodule to diagnosis of cancer was 3 years. A history of residence in an endemic goiter zone during the first decades of life is also relevant and must raise the possibility of multinodular goiter as the true diagnosis.
PHYSICAL FINDINGS
The adenoma is typically felt as a discrete lump in an otherwise normal gland, and it moves with the thyroid. Enlarged lymph nodes should be carefully sought, particularly in the area above the isthmus, in the cervical chains, and in the supra- clavicular areas. Their presence suggests malignant disease unless a good alternative diagnosis is apparent, such as recent oro-pharyngeal sepsis or viral infection. Fixation of the nodule to strap muscles or the trachea is alarming. Characteristically a benign thyroid adenoma is part of the thyroid and moves with deglutition, but can be moved in relation to strap muscles and within the gland substance to some extent. Pain, tenderness, or sudden swelling of the nodule usually indicates hemorrhage into the nodule but can also indicate an invasive malignancy. Hoarseness may arise from pressure or by infiltration of a recurrent laryngeal nerve by a neoplasm. Obviously the presence of a firm, fixed lesion, associated with pain, hoarseness, or any one of these features, should signal some degree of alarm. The converse situation, the absence of such characteristics, suggests but does not prove benignity. Fluctuance in the lesion suggest the presence of a cyst that is, usually, benign.
The presence of a diffusely multinodular gland, ascertained on the basis of palpation, US, or scanning, has in past years been interpreted as a sign of safety. Multinodular goiters coming to surgery have a significant prevalence of carcinoma (4-17%), but this finding was believed to be due largely to selection of patients for surgery, and not to be typical of multinodular goiters in the general population (31,32). However, in an era of generalized iodine sufficiency, when multinodular goiters are less common, this opinion needs re-evaluation. Frates et al (32.1) evaluated outcome in 1985 patients who underwent 3483 FNAs. Solitary nodules had the expected higher incidence of cancer than non-solitary nodules. However on a "per patient" basis, patients with MNG had the same incidence of diagnosed cancer (14.9%) as did patients with a solitary nodule (14.8%). Male sex, non-cystic nature, hypo-echogenicity, and stippled calcifications were associated with increased risk of malignancy per nodule. Usually FNA has been recommended for dominant or growing nodules. Frates et al recommend that for exclusion of malignancy in a thyroid with multiple nodules larger than 10mm, up to four nodules should be considered for FNA, and that the risk factors noted above may guide selection of nodules for biopsy.
Occasionally the gland has, in addition to a nodule, the diffuse enlargement and firm consistency of chronic thyroiditis, a palpable pyramidal lobe, and antibody test results that may be positive. These findings strongly suggest thyroiditis but do not disclose the nature of the nodule, which must be evaluated independently. It should be remembered that 14 - 20% (30, 33) of thyroid cancer specimens contain diffuse or focal thyroiditis. In addition, a positive association of thyroid cancer and Hashimoto's thyroiditis has been reported, but is not proven (v.i.).
Thyroid function tests
The patient is usually euthyroid, and this impression is supported by normal values for the serum FTI and T3 levels. Thyrotoxicity produced by an adenoma is discussed below. Low free thyroid hormones or elevated TSH results should raise the question of thyroiditis.
Curiously, it has been observed and confirmed that there is a direct correlation between TSH levels in patients with nodules and the risk of thyroid malignancy, and also with the degree of aggressiveness of the tumor(33.1)
The serum TG concentration may be elevated, as in all other goitrous conditions, and therefore is not a valuable tool in differential diagnosis. Calcitonin assay is indicated in the presence of a suggestive family history or of coincident features of the MEN-II syndromes. A chest x-ray should be taken if a normal film has not been reported in the prior 6 months. Soft tissue x-ray films of the neck may disclose indentation or deviation of the trachea if the tumor is more than 3 or 4 cm in diameter. Fine, stippled calcifications through the tumor (psammoma bodies) are virtually pathognomonic of papillary cancer. Patchy or "signet ring" calcification occurs in old cysts and degenerating adenomas, and has no such connotation.
Calcitonin assays
Although MTC constitutes a small fraction of thyroid malignancies, and an even smaller proportion of thyroid nodules, several reports suggest that routine screening of nodular goiters by CT assay is an appropriate approach (34-37). Such screening offers the possibility of finding tumors before they have metastasized, and MTC is rarely found on FNA. Whether the considerable expense is justified is yet indeterminate. Routine screening has been adopted as a standard procedure for evaluation of nodules in many clinics in Europe, but not in the USA. While calcitonin levels above 60 typically signal the presence of Medullary cancer, abnormal levels between 10 and 60 may be present with C-cell hyperplasia or no objective abnormality, and may spontaneously normalize(37.1).
FINE NEEDLE ASPIRATION CYTOLOGY
For many years core needle biopsy of the thyroid was employed successfully in some clinics to provide a histologic diagnosis on which to base therapy (38). Difficulties in acceptance of the procedure by surgeons, patients, and pathologists prevented its widespread application. As an alternative technique, thin needle aspiration cytologic examination has been widely adopted after favorable reports by Walfish et al (39) and Gershengorn et al (40). The procedure is technically simple and acceptable to patients, but requires an experienced operator and collaboration with a skilled cytopathologist (Figure 18-1). Two to four aspirations of the nodule, in different areas of the nodule, are recommended by many expert cytologists, particularly when the nodule is large enough (41). One common technique for sampling the whole nodule, is to introduce the needle in the center of the nodule, aspirate and then move the needle in another direction and aspirate again. The technique of FNA, and US-guided FNA, is described above in Chapter 6.
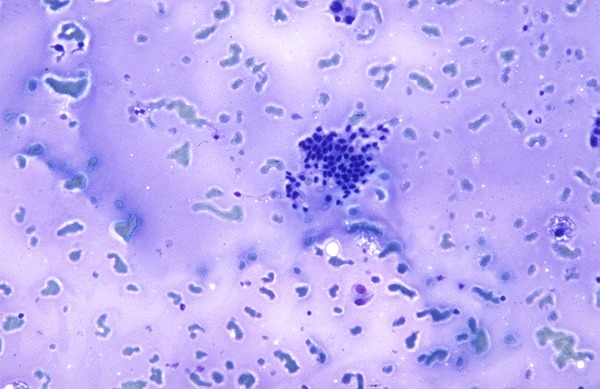
Fig 18-1a. Benign colloid nodule, showing scattered bits of coloid, few RBCs, and normal follicular cells
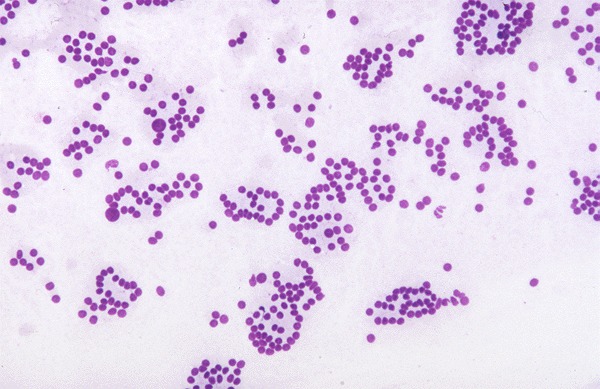
Figure 18-1B Epithelial cells in a follicular arrangement suggesting adenoma, but which could be from a follicular carcinoma.
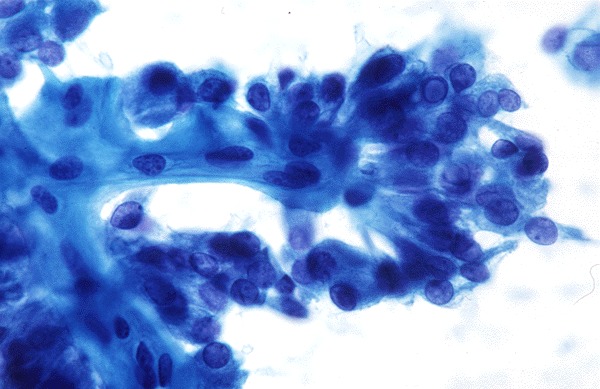
Figure 18-1C Epithelial cells in a papillary formation from a papillary thyroid carcinoma. Nuclear grooves are also apparent. (Courtesy of Dr. Richard DeMay, University of Chicago/Chicago Lying-in Hospital)
Significant complications such as bleeding, infection, induced necrosis, or cyst formation are rare. Surprisingly the release of thyroglobulin into the blood stream appears to induce development of anti-thyroxine antibodies, of IgG or IgM class, in some (2-20%) patients, especially those with prior evidence of autoimmune thyroid disease (42). Adequate specimens can be obtained in over 90% of patients. False-negative and false-positive diagnoses do of course occur, but are each under 5% with experienced hands. Willems and Lowhagen (43), in reviewing a collected series of nearly 4,000 surgically proven fine needle aspiration studies, found that 11.8% were considered to be malignant lesions. False-negative diagnoses of cancer were made in 6.6-27.5% and false-positive diagnoses in only 0-2%. Currently the results of FNA are viewed as the "gold standard" for diagnosis in most cases, and play a crucial role in the selection of patients for operation. Gharib and co-workers recently analyzed data on 10,000 FNAs, and found the procedure to be the preferred first step in diagnosis (44). The diagnostic accuracy was nearly 98%, with under two percent false positives and false negatives. Miller et al.52 compared fine needle aspiration, large needle aspiration, and cutting needle biopsy. They found fine needle aspiration cytologic examination was able to detect almost all carcinomas, but believe that cutting needle biopsy is a useful additional procedure, especially in larger (over 2-3 cm) nodules. A word of caution comes from a study by Tee et al, who reviewed published studies and concluded that FNA may miss up to a third of all thyroid malignancies (44.1)
A particular problem is posed when cytology discloses a follicular proliferation or a Hurthle celll proliferation. FNA cannot differentiate follicular adenoma from follicular carcinoma, since this distinction can only be based on the presence of capsular or vascular invasion, which cannot be detected on a cytologic smear. In these cases, the histological verification of the lesion is common, even though only 10-20% of nodules with follicular histology are proven to be malignant. An additional indication for FNA is the diagnostic evaluation of extra-thyroidal neck masses, especially lymph nodes, both at presentation and when the diagnosis of thyroid carcinoma has already been established. In these cases FNA may be integrated with the measurement of thyroglobulin content in the liquid recovered after washing the needle. If the lesion is metastatic from a differentiated thyroid cancer, thyroglobulin concentrations are very high (45).
In our practice, 5-8% of aspirates are found diagnostic of malignancy, 10-20% are considered suspicious (including those with follicular proliferation) but not diagnostic, 2-5% fail to provide an adequate specimen, and the remainder are considered benign, usually suggestive of a "colloid nodule" or thyroiditis. An inadequate specimen should lead to reaspiration. In a recent review of 153 patients with nondiagnostic FNAs, 60 patients had reaspiration. Of these 38% remain nondiagnostic. Of the group that went to operation, 37% had a malignancy. The authors conclude that nondiagnostic FNAs should not be considered benign, and that reaspiration, if uninformative, should be followed by selective surgical treatment (46). Non-palpable nodules can be biopsied under ultrasound guidance. Non-palpable thyroid nodules, typically < 1 cm in size, are usually non-malignant. It is uncertain whether ultrasound guided fine needle aspiration biopsy is appropriate in these individuals. However, considering that 4% are reported to be papillary cancers when diagnosed under ultrasound guidance, probably most careful physicians will elect to do such a biopsy, if possible (47). Of course a positive diagnosis of cancer leads to surgery. We, as others, tend to operate on patients with suspicious FNA histology, since about 25% prove at surgery to be malignant. In the remainder, continued observation and replacement thyroxine therapy are offered (v.i.). Patients who are not operated are seen at 6 or 12 month intervals, and examined for any sign such as pain, growth, hoarseness, or nodes that might indicate a change in the character of the tumor. Patients are usually re-biopsied after 2-3 years and possibly again after 5-8 years to document the benign nature of the lesion. The outcome of reaspiration of benign nodular thyroid disease was investigated by Erdogan et al in studies on more than 200 patients (48). Three of 216 patients had a diagnosis changed from benign to papillary carcinoma at the time of the second biopsy. The authors conclude that a second aspiration of clinically suspicious nodules can correct some initial false negative results, but routine reaspiration was not useful in clinically stable disease. A variety of techniques have been applied to improve accuracy of interpretation of FNA cytology or histology. Staining with antibodies to TPO and TG, or to T cell antigens, is fairly routine.
GENETIC DIAGNOSIS
Thanks to great technological advances, our understanding of the genomics of thyroid cancer has dramatically improved in last years. A number of mutations have been demonstrated in differentiated thyroid cancers and some of them are considered driver mutations for a specific cancer histotypes, often configuring a genotype-phenotype relationship. The MUC1 gene, and telomerase activity, are highly expressed in carcinomas rather than in adenomas in operative specimens (49, 49a). Overexpression of cyclin D1 and underexpression of p27 predict metastatic behavior in papillary nodules (49b). Expression of c-MET, galectin, VEGF, cathepsin B, thymosin, and HMG1 has been correlated with increased probability of malignancy. Dipeptidyl aminopeptidase IV activity is almost universally present in follicular carcinomas, and usually negative in adenomas (49c).
Published studies have clearly demonstrated that the most important driver genetic events of papillary and follicular thyroid cancer, respectively, occur in the MAPK and PI3K–AKT pathways. In this view, several reports have shown the validity of using a panel of oncogenes including at least BRAF, RET/PTC, PAX8/PPAR, RAS isoforms and hTERT mutations with possible addition of TRK rearrangement (50-50c). The main effect was due to determination of BRAF V600E mutation, which is present in 50-80% of papillary cancers. However cytologic diagnosis of papillary cancer is itself very accurate and BRAF identification would primarily help in a few uncertain cases. Nikiforev et al (50) found that in each of the indeterminate categories (using the Bethesda classification), atypia of undetermined significance/follicular lesion of undetermined significance, follicular or oncocytic Hurthle cell neoplasm, and suspicious for malignant cells, addition of the mutation screening changed diagnostic accuracy from 14-54%, up to 88-95%. A more comprehensive analysis is offered by the next-generation sequencing (NGS) approach which is able to interrogate multiple genes simultaneously in a cost-effective way with high sensitivity and working with low input of starting material (50d-50h).
Diagnosis by determining expression of relevant genes using gene microarray technology logically should be informative, since expression profiles of hundreds of genes can be analyzed at one time. Studies using the methodology on samples derived from FNA are currently being reported, although none has as yet reached practical clinical utility. Durand et al analyzed the level of expression of 200 potentially informative genes in 56 thyroid tissue samples (benign or malignant tumors and paired normal tissue) using nylon microarrays. Expression patterns of a series of 19 genes allowed discrimination between follicular adenomas+normal tissue, from follicular thyroid and papillary thyroid carcinomas. The procedure is believed applicable to the material collected by FNAB, but needs testing in a prospective study (51).
Several studies (51a-51g) addressed the issue whether the search of miRNAs in cytological material can refine FNAC diagnosis specially in indeterminate lesions since miRNAs can be easily extracted from fresh FNAC sample or from residual cells left within the needle cup. Generally, all the studies concluded that a set of miRNAs seems to be more sensitive than single miRNA and show consistent results in terms of diagnostic odd ratio (mean 20.3) but inconsistent data in terms of set of miRNA proposed. Future prospective and retrospective research are recommended on a large cohort of indeterminate lesions to validate the diagnostic value of miRNA in FNAC.Basically, we still wait a proven genetic diagnostic technique that can be applied to FNA samples with near-perfect reliability and accuracy. However, screening for mutated BRAF, RAS, RET/PTC and PAX8/PPRgamma, has already successfully become a part of routine examination of thyroid nodule cytology in some clinics.
Nishino (51h ) has recently provided an excellent description and comparison of the current commercially- available methods for classifying thyroid fine-needle aspirates by molecular techniques, especially those in the category of “atypia of undetermined significance/follicular lesion of undetermined significance” (AUS/FLUS) with a 5% to 15% risk of malignancy, and the “follicular neoplasm/suspicious for follicular neoplasm” (FN/SFN) category typically associated with a 15% to 30% risk of malignancy. The Afirma Gene Expression Classifier (GEC) and Afirma BRAF use microarray technology to assess the mRNA expression profiles of cytologically indeterminate thyroid nodules.The test is designed to “rule out” malignancy with a high PPV and low NPV, and is most clearly applicable to aspirates in the FN/SFN category, and may be less useful for AUS/FLUS aspirates. ThyGenX test is designed to “rule in” a possible diagnosis of malignancy by assaying FNA sample DNA for the most common oncogenic mutations in BRAF, KRAS, HRAS, NRAS, and chromosomal translocations resulting in RET/PTC1, RET/PTC3, and PAX8/PPARc fusions. Positive assay for BRAFV600E mutations and Ret/ PTC rearrangements carry a very high PPV. ThyroSeq V2 is similarly directed to “rule in” diagnosis of a malignancy. It uses parallel “next generation sequencing” targeted multiple portions of the genome in parallel searching for gene mutations in PIK3CA, PTEN, TP53, TSHR, CTNNB1, RET, AKT1, and TERT, as well as gene fusions involving RET, BRAF, NTRK1, NTRK3, AKT, PPARc, and THADA. It is also probably most useful on samples in the FN/SFN category, and less reliable in the AUS/FLUS category. Please consult this reference for extensive data on test performance.
Guidelines published by AACE and AME (51i) in January 2016 on management of thyroid nodules offers a wealth of carefully researched information. The authors advise that Molecular Testing should be considered to complement cytologic evaluation, and is appropriate if the results are expected to change therapy.The studies should include the detection of BRAF and RET/PTC and, possibly, PAX8/PPARG and RAS mutations if such detection is available. This group also concluded that there is “insufficient evidence to recommend use of gene expression classifiers (GECs) for decisions on cytologically indeterminate nodules”, that with the exception of mutations such as BRAFV600E, molecular evidence is insufficient to determine the extent of surgery , and that patients with nodules that are negative on mutation testing should still be monitored by close follow-up. Please consult this reference for a full description of their views,
THYROID ULTRASOUND
It is accepted practice to perform ultrasound examination of all thyroid nodules as the first study, or in conjunction with FNA. Good technique demonstrates nodules if more than 3 mm in size, indicates cystic areas, may demonstrate a capsule around the nodule, and the size of the lobes. (Fig 18-2) It often displays multiple nodules when only one is noted clinically. The technique is more sensitive than scintiscanning, is noninvasive, involves less time, allows serial exams, and is usually less expensive. From 3-20% of lesions are found to be totally or partially cystic. Purely cystic lesions are reported to have a lower incidence of malignancy than solid tumors (3% versus 10%), and diagnosis of a cyst raises the possibility of aspiration therapy (52). Mixed solid and cystic lesions allegedly have a higher frequency of malignant change than either pure cysts or solid lesions. While US can not diagnose malignancy, certain features such as irregular borders of the nodule, lack of a "halo", hypo-echogenicity, evidence of calcium flakes, marginal nodules in a cyst, increased blood flow, and growth on serial ultrasounds, are suggestive signs. Schlumberger and coworkers found that cystic appearance, hyperechoic punctuations, loss of hilum, and peripheral vascularization were major ultrasound criteria of lymph node malignancy. LNs with hyperechoic punctuations are highly suspicious of malignancy. LNs with a hyperechoic hilum should be considered benign. Peripheral vascularization has the best sensitivity-specificity compromise. Round shape, hypoechogenicity, and the loss of hilum taken as single criteria are not specific enough to suspect malignancy (52.1). Ultrasound gives also valuable information on the extranodular thyroid tissue, that may be useful for the differential diagnosis: a typical pattern of diffuse hypoechogeneity is almost synonymous with autoimmune thyroiditis (53).
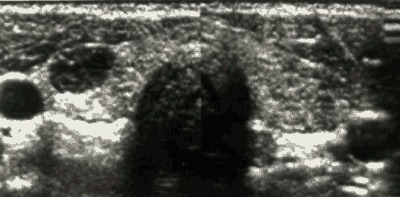
Figure 18-2.Ultrasooigraphic examination by transverse image of the thyroid containing a solid nodule in the left lobe and a homogeneous appearance of the right lobe. The structure peripheral to the nodule is the internal jugular vein.
A current problem is the proper way to manage thyroid nodules found incidentally on ultrasounds or CAT scans done for other purposes. As noted above, US-detectable nodules are present in a large proportion of all adults- perhaps 20 % as an average figure. If these are actually palpable, they fit into the schema just outlined. Whether to do US guided FNA on all non-palpable nodules, those generally smaller than 1cm and often as small as 3-5mm, is a question not clearly answered. Many patients request biopsy because they are anxious about the problem. Some studies have indicated that the incidence of carcinoma in these clinically non-detectable nodules is effectively the same as in larger nodules. At present our operational approach is to attempt biopsy in nodules 5-10 mm in size, and base treatment on the results. In smaller nodules or those judged very difficult to sample, the patient is advised to have repeated follow-up by exam and US at 6-12 month intervals. In a study of this problem by Papini et al 7% of nodules under 1 cm in size were found to harbor carcinomas. These authors believe that FNA is generally indicated, and especially if the nodule is solid and hypo-echogenic, has irregular margins, intranodular vascular spots, or microcalcifications.
ISOTOPE SCANS
The scintiscan received much attention in the past as an aid in the differential diagnosis of thyroid lesions (Chapter 6). The scan can provide evidence for a diagnosis in a multinodular goiter, in Hashimoto's thyroiditis, and rarely in thyroid cancer when functioning cervical metastases are seen. If the scan demonstrates a hyperfunctioning nodule suppressing the remainder of the gland, and the patient is thyrotoxic as demonstrated by an elevated serum FT4 or FT3 level, or suppressed sTSH, the chance of malignancy is very low. Tumors that accumulate RAI in a concentration equal to or greater than that of the surrounding normal thyroid tissue, but that do not produce thyrotoxicosis, are also typically benign (54, 55). In fact, some observers insist that functioning nodules cannot be malignant (55), in spite of reports of malignant change in occasional warm or hot nodules (55-59). Malignant tumors usually fail to accumulate iodide to a degree equal to that of the normal gland. However, most cold nodules turn out to be benign adenomas and cysts, not cancers. (Figure 18-3, below) The reported incidence of cancer in cold nodules is highly variable; a review of 400 cases found 10% to be cancer (60), and this experience is typical. Tumors smaller than 1 cm in size are below the discriminating power of most of the available scanning devices. Thus, a nodule 1 cm or less in diameter that fails to collect RAI (cold nodule) might not be delineated at all on the scintiscan. Further, many nodules turn out to be neither cold nor hot (preferential isotope accumulation); rather, they accumulate RAI in approximately the same concentration as the surrounding thyroid tissue. Normal tissue in front of or behind the nodule may also accumulate isotope and in this way obscure a deficit in collection within the lesion itself. For all of these reasons, it is our impression that the thyroid scintiscan has value, but except for the clearly toxic nodule, does not form an absolute predictor as to whether a palpable nodule is malignant or benign. Usually pertechnetate scanning provides the same information as RAI scanning, but exceptions occur. The first-line diagnostic procedures consist of ultrasound and TSH measurements. Thyroid scan is applied to autonomously functioning nodules and FNA to all the other nodules either cystic or solid or mixed.
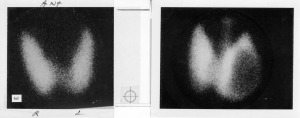
Fig. 18-3. Scintiscans of thyroid. The scan on the left is normal. A typical scan of a "cold" thyroid nodule failing to accumulate iodide isotope is shown on the right. Incidentally, a pyramidal lobe is also seen on this scan, which might suggest the presence of Hashimoto's Thyroiditis.
Several alternative isotopes, such as selenomethionine, radioactive phosphate, gallium, and technetium-labeled bleomycin, have been introduced for scanning, but none has proven to give clear cut evidence of malignancy or to be diagnostically superior to FNA. The same is true for other imaging techniques such as thyroid thermography, CT scan or MRI. All these techniques should not be used in daily clinical practice. Interestingly, fluorodeoxyglucose-PET scanning for other purposes occasionally turns up a hot spot in the thyroid.. On examination these thyroid nodules have a high rate of malignancy (61).
While FNA clearly has reduced the initial incidence of surgery in the management of nodules, the long term effect is less clear. Over three years of follow-up, at least 30% of our patients, who are believed to have a benign nodule, eventually undergo surgery. This occurs because they, or their physicians, remain concerned about the nodule, or the nodule is painful or grows, or is cosmetically unsatisfactory. But in most cases operation probably occurs because the patient cannot be entirely reassured by the physician that the lesion is safe.
THE DECISION FOR SURGERY
All thyroid nodules once discovered should undergo a complete diagnostic evaluation, regardless of the presenting manifestation or size. This allows the selection of patients with nodules that are malignant or suspicious of malignancy and therefore eligible for surgery. In addition, surgical treatment may be needed for some benign nodules, either single or associated with multinodular goiter, when they are large or associated with signs and symptoms of compression, discomfort, or for cosmetic concerns. All the other nodules are candidates either for medical therapy or simply follow-up with no therapy. A simple and practical flow-chart for the management of thyroid nodules, based on the results of the diagnostic evaluation is offered in Fig.18-4.
What is the prognosis, with or without treatment, for these thyroid malignancies? The majority are papillary or mixed papillary-follicular tumors, with fewer pure follicular and rare solid or anaplastic carcinomas. In general, the death rate due to thyroid carcinoma, 5-6 per 10-6 persons per year in the USA in reported by the SEER program and possibly 6/million/year indicated recently, is approximately 5% of the incidence rate of 110 per million people each year (62, 63, http://seer.cancer.gov/statfacts/html/thyro.html.). (Incidence rates are 160/10-6 women and 56/10-6 men) Although it would be comforting to believe that the difference between the incidence and death rates is due to the effectiveness of surgical and medical therapy, it also reflects the remarkable benignity of many of these tumors. Some patients carry them throughout their lives and die from other causes. Although no controlled series is available, it seems obvious that some carcinomas that occur first as nodules will cause death. About all that can be stated with certainty is that some patients do die from thyroid carcinoma, and that if the surgeon removes a nodule that is really an invasive tumor before it has metastasized, or while it is still under the control of the defense mechanisms of the body, a cure is effected.
THERAPY FOR NODULES (Table 18-3,18-4) (Figure 18-4)
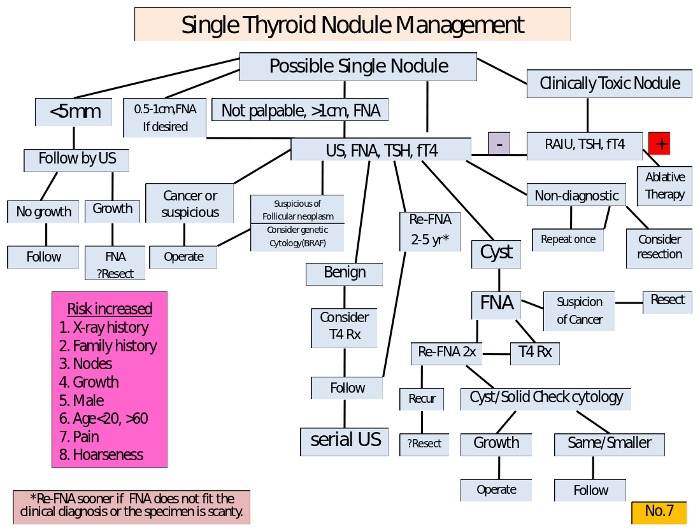
Figure 18-4Diagnostic sequence and therapeutic decisions in managing a patient with an apparent single nodule of the thyroid.
Toxic Nodules
Three therapeutic options are available for toxic nodules: surgery, 131-I therapy and ethanol injection. Antithyroid drugs can be used if necessary prior to definitive therapy, for example during pregnancy. Radioiodine is a very effective therapy and is becoming the treatment of choice in most patients over 21 years of age and particularly in older patients and those with coincident serious illness, because of its ease and convenience, slightly lower expense, avoidance of a scar, and avoidance of hospitalization. The activity of 131-I to be administered will depend on the size of the nodule and usually ranges between 185 and 740 MBq (5-20 mCi). Euthyroidism and a variable shrinkage of the nodule are obtained in most patients. When one single dose is ineffective, the procedure may be repeated. With time, hypothyroidism may develop in up to 30-40% of the patients, since the remainder of the gland receives 1,000-8,000 rads (64). Hypothyroidism is more frequent in patients with positive anti-thyroid autoantibodies prior to therapy (59a). Further, the patient receives 30-60 rads of whole body irradiation (65). Although, in theory, this radiation could induce cancer formation, this has not been reported.
Surgery is indicated for large nodules, particularly when they have a large cystic component, in very young patients (although rare) and in those refusing radioiodine therapy. Surgery consists of a total lobectomy and must be performed after restoration of a normal thyroid function by antithyroid drugs. Also after surgery, late hypothyroidism is common (30-40% in our experience), while the occurrence of surgical complications is nearly absent in the hands of experienced surgeons.
The third option for the treatment of toxic or pre-toxic nodules, ethanol injections, has been proposed by Italian authors (66, 67). The procedure consists in percutaneous intra-nodular ethanol injection, which induces cellular dehydration followed by coagulative necrosis and vascular thrombosis and occlusion. Volumes of .4 - 2 ml are injected, and patients may receive up to 9 or more treatments at intervals of several days. The technique requires a well-trained staff. Transient, sometimes severe, local pain is the most frequent side effect, followed by transient fever, and occasionally transient dysphonia. Long term follow-up studies have shown that the rate of recurrence is limited to a few patients, and almost no patient developed hypothyroidism (68). However, in our opinion, this therapeutic option should be limited to highly selected cases, such as small nodules, well accessible to palpation, in patients at surgical risk or refusing radioiodine. Small autonomous functioning thyroid nodules, without thyrotoxicosis, can be left untreated and followed. Nearly 30-40% will eventually evolve into toxic nodules (69), but many may stay as they are or even undergo spontaneous cystic degeneration.
Cysts
Cystic lesions are aspirated and often reaspirated one or more times. Possibly long-term replacement with thyroid hormone tends to prevent recurrence, although this outcome is uncertain (70). If, after repeated aspiration, the lesion is still clearly evident, it must be considered a mixed solid/cystic lesion and probably should be resected. Cytologic examination of the aspirated fluid should be done, but the specimens are often not satisfactory for diagnosis. Some physicians attempt to sclerose cysts by aspirating fluid, and then reinjecting one-half volume of a 10/1 mixture of saline and an injectable form of tetracycline containing 100 mg/ml of the drug. Care must be taken to avoid subcutaneous leakage which is very painful. The technique is not widely used, but is reported to be effective (71). Sclerotherapy by ethanol injection is an other promising method of treatment for thyroid cysts. A major reduction in cyst volume, with very low rate of recurrence has been reported in two publications (72, 73). Large cysts (over 40 ml volume) can also be treated by ethanol injection in several sessions with > 50% reduction in size in most cases (74).
Solid nodules
Solid, mixed, functioning, or "cold" nodules constitute the remaining group and indeed the majority of cases. Here major reliance is placed on aspiration cytology. If the results are positive for carcinoma, resection is offered. If no specimen is obtained, reaspiration is performed. If the specimen is suspicious, reaspiration or resection is mandatory. Usually "suspicious" cytology and follicular proliferation leads to resection, since about 25% of nodules with this cytological picture are carcinomas at final pathology
Table 18-3Factors to be Considered in Management of Cold Nodules
| History | Physical Examination | Laboratory tests |
|---|---|---|
| Radiation | Size | FTI |
| Age | Fixation | Antithyroid antibodies |
| Sex | Cystic nature | TG |
| Duration | Tenderness | Chest Xray film |
| Local Sysmptoms | Adenopathy | Fine needle aspiration |
| Growth | Diffuse/local process | Ultrasound scan |
| MEN Syndrome | Vocal cord paralysis | ?) Isotope scan |
| Thyrotoxicity | Single vs multiple | ?) Xray soft tissues of neck |
| Geographic residence | ||
| Family History |
THYROXINE TREATMENT
If a benign result is obtained on cytologic examination, the patient is followed intermittently and may, or may not, be given mildly "suppressive" doses of thyroxine. There is no unanimity on the value of this treatment, and many endocrinologists do not believe thyroid therapy is useful. However solid evidence for the value (modest) of the treatment, and lack of problems, is gradually accumulating. Patients are given thyroxine in a dose adjusted to keep TSH in the minimally depressed range -- e.g. 0.1-0.3 µU/ml. (Fig. 18-5, below) It is recognized that the efficacy of this treatment to shrink nodules is modest, but it does appear to reduce the size of 10-20% of the lesions (75-79), may prevent further growth, and keeps patients under obseervation.. Meta-analyses of studies on thyroid hormone suppressive therapy for solitary thyroid nodules were presented by Castro et al (80) and Zelmanovitz et al (81). A 50% reduction in nodule volume was found in 17% more of T4-treated patients than those left untreated, and nodule volume increased more than 50% in a larger proportion of untreated patients. Nodules which are recent, small, colloid or showing degenerative changes at cytology are those more prone to respond to thyroxin treatment (82,83). An almost identical result (84) was found in a randomized, double-blind, placebo controlled study done by a group of French clinicians, who also noted that thyroxin treatment dramatically reduced the number of newly recognized nodules during follow-up. Sdano et al (83a) did a meta-analysis of 9 randomized studies, with 609 subjects.Subjects were 88% more likely to experience >50% nodule volume reduction with THST than placebo or no treatment (relative risk = 1.88; 95% CI = 1.18-3.01; P = 0.008). However studies with follow-up after thyroxine withdrawal demonstrate rapid increase in thyroid nodule and goiter volumes, and these authors did not advise routine use for benign nodules. Age is also important in the selection process. We prefer to treat young adult patient up to 60 years of age. In older patients therapy must be considered on an individual basis, after excluding other underlying chronic diseases, such as heart problems. If a patient is already on L-T4 and has a good compliance with no side effects, treatment may be continued after 60 years, slightly reducing the daily dose. In case of multinodular goiter, a condition frequently associated with intra-glandular areas of functional autonomy, particular attention should be paid to the TSH pre-treatment level. If this is already in the low-normal range, as frequently seen, it is advisable to start l-T4 at very low daily doses (25 µg/day), increasing the dose gradually according to the TSH modifications, to avoid iatrogenic thyrotoxicosis. The level of hormone replacement is chosen in the belief that it is unlikely to cause symptoms of hyperthyroidism, such as palpitations, and unlikely to cause osteoporosis, even with prolonged use, while presumably does reduce growth stimulation to the nodule.The usual l-T4 dose is 1 - 2.0 µg/Kg/day, to be administered in the morning and while fasting. The appropriate dose should be checked by measuring FT3 and TSH, 3-4 months after its institution. Normal free T3 values exclude significant over-treatment, even when FT4 is in the upper limit of normal.
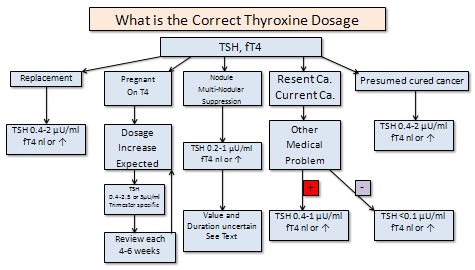
Fig. 18-5-Correct thyroxine treatment
It is not appropriate to maintain postmenopausal women, on doses of hormone that produce even mild hyperthyroidism for a long period, in view of the potential induction of osteoporosis and arrhythmias. However it should be noted that prolonged suppression of TSH to about 0.1uU/ml by T4 doses just above physiological in premenopausal women does not appear to induce bone loss, nor is it certain that this therapy increases fracture risk in older women (85). Serum TG is usually measured at each visit. Suppression of TG to a normal level by T4 therapy is a gratifying and reassuring response, and is correlated with nodule shrinkage (86). Progressive elevation suggests resection should be considered.
Patients receiving thyroxin therapy, or not, are followed indefinitely at 6- to 12-month intervals, and future management varies with the patient's course. Adverse factors to be noted include growth, development of local symptoms, or adenopathy. In all patients under age 25, all men, and those with a history of neck irradiation, any change usually constitutes grounds for resection. In women 25 years of age and up, the situation should be carefully reviewed and reaspiration performed. If the changes can be explained in the context of a benign process and the reaspirate is benign, continued careful medical follow-up is acceptable, but operation will often be preferred by the patient or physician. The desired course in follow-up is for a gradual reduction and disappearance of the offending lesion. Although this result occasionally is seen, most often the lump remains the same or a bit smaller and persists year after year.
Table 18 - 4Management of Nodules
| Category | Aspiration Data | Management |
|---|---|---|
| Thyrotoxic hot nodule | Lobectomy, or 131I therapy, or (?) sclerotherapy | |
| "Mainly cystic | Aspirate for Dx and therapy; reaspirate as needed | T4 therapy; resection; (?) sclerotherapy |
| Other nodules | Probable cancer | operate |
| Inadequate specimen | reaspirate | |
| Benign | follow with/with out T4 therapy and periodic exam , US, and FNA | |
| Suspicious or hypercellular | Probably operate |
SURGICAL RESECTION
The most important requirement for surgery is the selection of an experienced surgeon in an institution with an adequate Department of Pathology. The patient is occasionally pretreated for several weeks with of thyroid hormone to suppress the normal thyroid and thereby better delineate the nodule from the normal gland. The surgeon should be prepared to do a lobectomy if the lesion is benign, or a more extensive operation and appropriate lymph node removal if, from the operative findings and examination of frozen sections, it is malignant. If the lesion is described as a hypercellular follicular adenoma, we feel it is best to do a lobectomy and contralateral subtotal lobectomy. Many of these lesions turn out on final pathology to be malignant, and reoperation is then avoided.
The first operation is the time for definitive surgery. Although a surgeon with limited experience in neck surgery can remove a thyroid nodule, an adequate near-total thyroidectomy and modified radical neck dissection requires experience, if damage to the recurrent laryngeal nerves or induction of hypoparathyroidism is to be avoided. In this day of specialization, patients deserve a surgeon who has more than a casual interest in the field. Indeed, in the absence of such surgical skill, medical therapy may offer significantly fewer problems for certain patients with nodules than those arising out of inadequate surgery.
Lobectomy for benign solitary adenomas is a relatively harmless procedure. The incidence of death, recurrent laryngeal nerve paralysis, or permanent hypoparathyrodism should be zero. It is less of a procedure than is subtotal thyroidectomy for Graves' disease. Only 1-2 days are required in the hospital, and currently some surgeons do thyroid lobectomy as an “outpatient” proceedure.. Post-operative morbidity is slight and transient, and the cosmetic appearance is almost always satisfactory. Complications increase if a carcinoma is discovered, and thyroidectomy and node dissection are required. However, this risk is more than balanced by the benefits (87), since long-term survival after surgery for intrathyroidal or locally metastatic thyroid carcinoma is almost equal to that of the "normal" population.
A satisfactory outcome often depends on a pathologist competent in thyroid histopathology. Occasionally the difficulty of interpreting frozen sections will lead to thyroidectomy for a tumor that is ultimately classified as benign. Performance of an occasional unnecessary thyroidectomy is not a serious problem in the hands of a surgeon who has few operative complications. On the other hand, reoperation at a later date for cancer erroneously diagnosed at initial surgery as benign is all too often required, and does not offer the patient the best chance of operative cure and freedom from operative complications.
After operation many thyroidologists favor treating patients with long-term replacement therapy with thyroid hormone. Although the recurrence of "solitary" nodules is infrequent, replacement therapy is safe, inexpensive, and probably provides some protection. There is no general agreement on this point. We note that thyroxin treatment has been shown to decrease recurrence of nodules in patients operated for thyroid disease induced by childhood irradiation (88).
Occasionally, when the patient is recuperating from lobectomy for a presumed benign lesion, the permanent tissue sections indicate to the pathologist that the diagnosis is actually carcinoma of the follicular or papillary type. If the lesion is over 1 cm in size, there is a history of irradiation, or the lesion is follicular, completion of the thyroidectomy is advisable, as discussed below, since up to 30% of such re-operations disclose residual tumor. This is certainly appropriate if there is nodularity in the residual thyroid on US exam. An alternative approach is to ablate the residual lobe with 30 mCi of RAI, which is effective in eliminating most of the tissue. Although easy for the patient, and certainly free of surgical complications, whether this provides the same protection as re-operation is not known.
SCLEROTHERAPY
Bennedbaek and Hegedus have carefully evaluated percutaneous ethanol injection therapy in benign solitary solid cold thyroid nodules. Ninety-eight percent ethanol (25 – 50% of nodule volume) was injected under ultrasound guidance intending to achieve uniform spread throughout the nodule. The overall reduction in nodule volume at six months was 46 – 51%. While the majority of patients benefited from reduction in nodule size, significant side effects included transient thyrotoxicosis, permanent facial dysesthesia, paranodular fibrosis, pain, and tenderness. They conclude that the optimum strategy is yet uncertain and that the procedure is limited, especially by local pain and the significant number of side effects, so that caution is advisable in routine use (89).
Dossing et al treated 78 euthyroid outpatients with a benign solitary solid and scintigraphically cold thyroid nodule causing local discomfort, with Interstitial Laser Photocoagulation (ILP). using one laser fiber under ultrasound (US) guidance and an output power of 1.5-3.5 W. The overall median nodule volume decreased from 8.2 ml (range 2.0-25.9) to 4.1 ml (range 0.6-33.0; P<0.001) at the final evaluation. After 12--96 months (median 38 months) of ILP, 21 patients (29%) had thyroid surgery because of an unsatisfactory result..US-guided ILP results in a satisfactory long-term clinical response in the majority of patients with a benign solitary solid cold thyroid nodule, but further large-scale studies are needed (89.1).
THYROID NODULES IN CHILDREN
In areas of iodide deficiency diffuse thyroid enlargement is found during pre-teen years, and multi-nodularity commonly occurs by teenage. In contrast, in an iodide-replete country, discovery of a nodule in the thyroid of a child is (fortunately) uncommon, and always raises alarm because of the risk of neoplasia. There is a +/- 5% incidence of cancer in "single nodules" in adults, but up to 18% of those found in children are malignant. This high incidence raises the issue whether all such nodules should be immediately resected, or if it is legitimate to employ the available diagnostic tests to select those for whom surgery should be advised?
Nodules in children are infrequently cystic, perhaps because cystic nodules represent an end stage in some long standing benign growths. Of course cystic lesions can be malignant. We have observed that a significant proportion of enlarging thyroid masses in children produce hyperthyroidism and turn out to be "hyperplastic colloid nodules" on pathological exam, although there are reports that up to 1/4 of "hot nodules" in children are papillary cancers. The majority are inactive on isotope scanning, solid on ultrasound, do not produce hyperthyroidism, and are painless.
If there is rapid growth, if possibly related nodes are present or if there is any other suggestion of malignancy, or if the nodule is the apparent cause of hyperthyroidism, resection is inevitable. For the remaining patients, a question is whether to do a fine needle aspiration cytological exam, or offer resection without this examination. Many thyroidologists caring for pediatric patients would suggest resection directly, but the alternative position is to do an FNA, be guided by the results, and to follow the patient closely with resection in mind if any unfavorable sign occurs (90). Our attitude is to perform FNA in virtually all cases, the reason being not only the selection of therapy, but, even if surgery is already planned, to provide the surgeon with the most likely diagnosis, thus allowing better planning of the surgical procedure. Also, this approach is taken in view of the occasional false positive or false negative diagnosis by intra-operative pathological examination. Since the natural history of such nodules is to enlarge, many will ultimately come to operation. In these patients thyroxine treatment may have value as reported by Renshaw et al(90.1). These authors found in a study of 78 euthyroid children with benign nodules, that T4 threatment reduced size up to 50%, while untreated nodules typically enlarged.
The operative approach is comparable to that used in adults. If the nodule is definitively benign at surgical pathological exam and the remainder of the thyroid is normal, lobectomy or more limited resection is performed. If the lesion is a hypercellular follicular adenoma or if there is uncertainly in the exam, or if other nodules are found, a lobectomy and contra-lateral sub-total resection is often performed. Near-total thyroidectomy with/without node resection is done for malignancy.
INCIDENTALOMAS
Wide spread use of ultrasound for exam of any neck pathology has resulted in frequent recognition of thyroid nodules that are too small to be palpated on clinical examination. Usually such nodules are < 1cm in largest diameter, typically they are asymptomatic, and are not associated with lymph nodes or other suggestions of malignancy. Often incidentally found, such nodules produce a problem because of the difficulty in achieving a specific diagnosis, which is desired by the patient.
The usual differential diagnostic possibilities, described above, are present. The probability of malignancy is lower than in larger lesions, although exactly how much so is uncertain. In a recent meta-nalysis by Tan and Gharib (91), the risk for malignancy in incidentalomas ranged betwen 0.45% and 13%.Tiny cystic lesions are especially unlikely to harbor a malignancy. Presence of neck adenopathy, local symptoms such as pain or dysphonia, growth under observation, or a history of external radiation to the neck, signal concern and suggest that resection is the proper course.
If the lesion can be palpated it is appropriate to offer FNA cytological exam and proceed as for management of larger lesions. More typically the nodule can not be precisely demarcated on exam. Ultrasound guided FNA is possible for lesions closer to 1 cm in size, and in patients who clearly want every diagnostic assurance available. The smaller lesions are difficult to aspirate with certainty even under ultrasonic guidance. (See discussion above) Considering the probable benign nature of most such lesions, the slow growth and spread of differentiated thyroid cancers, and our ability to offer close surveillance via yearly (or more frequent) ultrasound exams, a common alternative course is "observe" tiny lesions periodically and reserve resection for those that grow or produce other symptoms.
Suppressive doses of thyroxin can be offered to patients being followed medically. It is clear that shrinkage can be anticipated in only a small fraction of lesions, but this treatment may help reduce future growth, provides a reason for the patient to remain under medical observation, and may, by shrinking the normal tissue, make the nodule palpable and thus more easily examined. Growth under observation and in the absence of cytological diagnosis, or development of nodes or local symptoms, indicate the need for resection.
REFERENCES
- Hedinger, C, Dillwyn Williams, E, Sobin, L 1989. The WHO histological classification of thyroid tumors. A commentary on the second edition. Cancer 63:908-9112.Namba, H, Matsuo, K, Fagin, J 1990 Clonal composition of benign and malignant human thyroid tumors. J Clin In 86:.3.Parma, J, Duprez, L, Van Sande, J, et al. 1993. Somatic mutations in the thyrotropin receptor gene cause hyperfunctioning thyroid adenomas. Nature 365:649-6514.Tonacchera, M, Chiovato, L, Pinchera, A, et al. 1998 Hyperfunctioning thyroid nodules in toxic multinodular goiter share activating thyrotropin receptor mutations with solitary toxic adenoma. J Clin Endocrinol Metab 83:492-85. Coclet, J, Foureau, F, Ketelbant, P, Galand, P, Dumont, J 1989. Cell population kinetics in dog and human adult thyroid. Clinical Endocrinol 31:655-6656. Viglietto, G, Chiappetta, G, Martinez-Tello, F J, et al. 1995 RET/PTC oncogene activation is an early event in thyroid carcinogenesis. Oncogene 11:1207-107. Hamburger, J I 1980; Evolution of toxicity in solitary nontoxic autonomously functioning thyroid nodules. J Clin Endocrinol Metab 50:1089-10938. Silverstein, G, Burke, G, Cogan, R 1967. The natural history of the auto-nomous hyperfunctioning thyroid nodule. Ann Intern Med 67:5399. Evered, D, Clark, F, Peterson, V 1974. Thyroid function in euthyroid subjects with autonomous thyroid nodules. Clin Endocrinol 3:14910. Horst, W, Rosler, H, Schneider, C, Labhart, A 1967. 306 cases of toxic adenoma. Clinical aspects; findings in radioiodine diagnostics; radiochromatography and histology; results of 131I and surgical treatment. J Nucl Med 8:51511.Parma, J, Duprez, L, Van Sande, J, et al. 1993. Somatic mutations in the thyrotropin receptor gene cause hyperfunctioning thyroid adenomas. Nature 365:649-65112.Suarez, H, du Villard, J, Caillou, B, Schlumberger, M, Parmentier, C, Monier, M 1991. Gsp mutations in human thyroid tumors. Oncogene 6:677-67913. see 1013a. DeGroot, L 1970. Lack of iodide trapping in "cold" thyroid nodules. Acta Endocrinol Panam 1:2714. Field, J, Larsen, P, Yamashita, K, Mashiter, K, Dekke, A 1973. Demonstration of iodide transport defect but normal iodide organification in nonfunctioning nodules of human thyroid glands. J Clin Invest 52:240415. Fragu, P, Nataf, B 1977. Human thyroid peroxidase activity in benign and malign thyroid disorders. J Clin Endocrinol Metab 45:108916. Demeester-Mirkine, N, Van Sande, J, Corvilain, H, Dumont, J 1975. Benign thyroid nodule with normal iodide trap and defective organification. J Clin Endocrinol Metab 41:116917. Burke, G, Szabo, M 1972. Dissociation of in vivo and in vitro "autonomy" in hyperfunctioning thyroid nodules. J Clin Endocrinol Metab 35:19918. Sande Van, J, Mockel, J, Boeynaems, J, Dor, P, Andry, G, Dumont, J 1980. Regulation of cyclic nucleotide and prostaglandin formation in normal human thyroid tissue and in autonomous nodules. J Clin Endocrinol Metab 50:77619. Smanik, P, Ryu, K-Y, Thel, K, Mazzaferri, E, Jhiang, S 1997. Expression; exon-intron organization; and chromosome mapping of the human sodium iodide symporter. Endocrinology 138:3555-820.Arturi, F, Russo, D, Schlumberger, M, et al. 1998. Iodine symporter gene expression in human thyroid tumors. J Clin Endocrinol Metab 83:2493-9621. Thomas, C J, Buckwalter, J, Staab, E, Kerr, C 1976. Evaluation of dominant thyroid masses. Ann Surg 183:46422. Sipple, J H 1984 Multiple endocrine neoplasia type 2 syndromes: historical perspectives. Henry Ford Hosp Med J 32:219-2123.Schimke, R, Hartmann, W, Prout, T, Rimoin, D 1968. Syndrome of bilateral pheochromocytoma; medullary thyroid carcinoma; and multiple neuromas. N Engl J Med 279:124.Sapira, J, Altman, M, Vandyk, K, Shapiro, A 1965. Bilateral adrenal pheo-chromocytoma and medullary thyroid carcinoma. N Engl J Med 273:14025. Duffy, B J, Fitzgerald, P 1950. Cancer of the thyroid in children. A report of twenty-eight cases. J Clin Endocrinol 10:129626. Clark, D 1955. Association of irradiation with cancer of the thyroid in children and adolescents. JAMA 159:100727. Modan, B, Ron, E, Werner, A 1977. Thyroid cancer following scalp irradiation. Therapeutic Radiology 123:74128 DeGroot, L, Frohman, L, Kaplan, E, Refetoff, S e 1977. Radiation-Associated Thyroid Carcinoma. New York Grune & Stratton:539 pages29. Refetoff, S, Harrison, J, Karanfilski, B, Kaplan, E, DeGroot, L, Bekerman, C 1975. Continuing occurrence of thyroid carcinoma after irradiation to the neck in infancy and childhood. N Engl J Med 292:17130 DeGroot, L, Paloyan, E 1973. Thyroid carcinoma and radiation. A Chicago endemic. JAMA 225:48731. Sokal, J 1959. The problem of malignancy in nodular goiter -- recapitulation and a challenge. JAMA 170:6132. Veith, F, Brooks, J, Grigsby, W, Selenkow, H 1964. The nodular thyroid gland and cancer. N Engl J Med 270:43132.1 Frates MC, Benson CB, Doubilet PM, Kunreuther E, Contreras M, Cibas ES, Orcutt J, Moore FD Jr, Larsen PR, Marqusee E, Alexander EK. Prevalence and distribution of carcinoma in patients with solitary and multiple thyroid nodules on sonography. J Clin Endocrinol Metab. 2006 Sep;91(9):3411-7.33. Hoffman, G, Thompson, N, Heffron, C 1972. The solitary thyroid nodule. Arch Surg 105:37933.1 Haymart MR, Repplinger DJ, Leverson GE, Elson DF, Sippel RS, Jaume JC, Chen H.Higher serum thyroid stimulating hormone level in thyroid nodule patients is associated with greater risks of differentiated thyroid cancer and advanced tumor stage.J Clin Endocrinol Metab. 2008 Mar;93(3):809-14.34. Pacini, F, Fontanelli, M, Fugazzola, L, et al. 1994. Routine measurement of serum calcitonin in nodular thyroid diseases allows the preoperative diagnosisof unsuspected sporadic medullary thyroid carcinoma. J Clin Endocrinol Mertab 78:826-935. Rieu, M, Lame, M, Richard, A, et al. 1995. Prevalence of sporadic medullary thyroid carcinoma. the importance of routine measurement of serum calcitonin in the diagnostic evaluation of thyroid nodules. Clin Endocrinol (Oxf) 42:453-736. Niccoli, P, Wion-Barbot, N, Caron, P, et al. 1997. Interest of routine measurement of serum calcitonin. Study in a large series of thyroidectomized patients. J Clin Endocrinol Metab 82:338-34137. Gagel, R 1997. The goitrous patient with an elevated serum calcitonin -- what to do? J Clin Endocrinol Metab 82:33537.1 Cherenko M, Slotema E, Sebag F, De Micco C, Henry JF. Mild hypercalcitoninaemia and sporadic thyroid disease. Br J Surg 2010 May:97 (5) :684-90
- Hamlin, E, Vickery, A 1956. Needle biopsy of the thyroid gland. N Engl J Med 254:74239. Walfish, P, Hazani, E, Strawbridge, H, Miskin, M, Rosen, B 1977. Combined ultrasound and needle aspiration cytology in the assessment and management of hypofunctioning thyroid nodule. Ann Intern Med 87:27040. Gershengorn, M, McClung, M, Chu, W, Hanson, T, Weintraub, B, Robbins, J 1977. Fine-needle aspiration cytology in the preoperative diagnosis of thyroid nodules. Ann Intern Med 87:26541.Baloch, Z, Sack, M, Livolsi, V, Gupta, P 1998. Fine-needle aspiration of thyroid. an institutional experience. Thyroid 8:565-942. Benvenga, S, Bartolone, L, Squadrito, S, Trimarchi, F 1997. Thyroid hormone autoantibodies elicited by diagnostic fine needle biopsy. J Clin Endocrinol Metab 82:4217-422343 Wilems, J-S, Lowhagen, T 1981. Fine needle aspiration cytology in thyroid disease. . Clin Endocrinol Metab 2:24744 Gharib, H, Goellner, J, Johnson, D 1993. Fine needle aspiration cytology of the thyroid. A 12-year experience with 11;000 biopsies. Clin Lab Med 13:699-70944.1 Tee YY, Lowe AJ, Brand CA, Judson RT.Fine-needle aspiration may miss a third of all malignancy in palpable thyroid nodules: a comprehensive literature review.Ann Surg. 2007 Nov;246(5):714-20.45. Pacini, F, Fugazzola, L, Lippi, F, et al. 1992 Detection of thyroglobulin in fine needle aspirates of nonthyroidal neck masses. a clue to the diagnosis of metastatic thyroid cancer. J Clin Endocrinol Metab 74:1401-446. Chow, L S, Gharib, H, Goellner, J R, van Heerden, J A 2001 Nondiagnostic thyroid fine-needle aspiration cytology: management dilemmas. Thyroid 11:1147-5147. Khurana, K, Richards, V, Chopra, P, Izquierdo, R, Rubens, D, Mesonero, C 1998. The role of ultrasonography-guided fine-needle aspiration biopsy in the management of nonpalpable and palpable thyroid nodules. Thyroid 8:51148. Erdogan, M, Kamel, N, Aras, D, Akdogan, A, Baskal, N, Erdogan, G 1998. Value of reaspirations in benign nodular thyroid disease. Thyroid 8:108749. Bieche, I, Ruffet, E, Zweibaum, A, Vilde, F, Lidereau, R, Franc, B 1997. MUC1 Mucin gene; transcripts; and protein in adenomas and papillary carcinomas of the thyroid. Thyroid 7:72549a Brousset, P, Chaouche, N, Leprat, F, et al. 1997. Telomerase activity in human thyroid carcinomas originating from the follicular cells. J Clin Endocrinol Metab 82:4214-421649b Khoo, M L, Beasley, N J, Ezzat, S, Freeman, J L, Asa, S L 2002 Overexpression of cyclin D1 and underexpression of p27 predict lymph node metastases in papillary thyroid carcinoma. J Clin Endocrinol Metab 87:1814-849c. Maruta, J; Hashimoto, H; Yamashita, H; Yamashita, H; Noguchi, S. Diagnostic applicability of dipeptidyl aminopeptidase IV activity in cytological samples for differentiating follicular thyroid carcinoma from follicular adenoma. Arch Surg 139 83-88 2004.50. Nikiforov YE, Ohori NP, Hodak SP, Carty SE, Lebeau SO, Ferris RL, Yip L, Seethala RR, Tublin ME, Stang MT, Coyne C, Johnson JT, Stewart AF, Nikiforova MN. Impact of Mutational Testing on the Diagnosis and Management of Patients with Cytologically Indeterminate Thyroid Nodules: A Prospective Analysis of 1056 FNA Samples. J Clin Endocrinol Metab. 2011;96:3390-7.
50a. Ferraz C, Eszlinger M, Paschke R.Current state and future perspective of molecular diagnosis of fine-needle aspiration biopsy of thyroid nodules. J Clin Endocrinol Metab. 2011;96:2016-26.
50b. Nikiforov YE, Steward DL, Robinson-Smith TM, Haugen BR, Klopper JP, Zhu Z, et al. Molecular testing for mutations in improving the fine-needle aspiration diagnosis of thyroid nodules. J Clin Endocrinol Metab, 94, 2092-2098 2009.
50c. Cantara S, Capezzone M, Marchisotta S, Capuano S, Busonero G, Toti P, et al. Impact of proto-oncogene mutation detection in cytological specimens from thyroid nodules improves the diagnostic accuracy of cytology. J Clin Endocrinol Metab;95: 1365-1369, 2010.
50d. Le Mercier M, D'Haene N, De Nève N, Blanchard O, Degand C, Rorive S, Salmon I. Next-generation sequencing improves the diagnosis of thyroid FNA specimens with indeterminate cytology. Histopathology. 2015;66:215-24.
50e. Nikiforova MN, Wald AI, Roy S, Durso MB, Nikiforov YE. Targeted next-generation sequencing panel (ThyroSeq) for detection of mutations in thyroid cancer. J Clin Endocrinol Metab. 2013;98:E1852-60.
50f. Hadd AG, Houghton J, Choudhary A, Sah S, Chen L, Marko AC, Sanford T, Buddavarapu K, Krosting J, Garmire L, Wylie D, Shinde R, Beaudenon S, Alexander EK, Mambo E, Adai AT, Latham GJ. Targeted, high-depth, next-generation sequencing of cancer genes in formalin-fixed, paraffin-embedded and fine-needle aspiration tumor specimens. J Mol Diagn. 2013;15:234-47.
50g. Kanagal-Shamanna R, Portier BP, Singh RR, Routbort MJ, Aldape KD, Handal BA, Rahimi H, Reddy NG, Barkoh BA, Mishra BM, Paladugu AV, Manekia JH, Kalhor N, Chowdhuri SR, Staerkel GA, Medeiros LJ, Luthra R, Patel KP. Next-generation sequencing-based multi-gene mutation profiling of solid tumors using fine needle aspiration samples: promises and challenges for routine clinical diagnostics. Mod Pathol. 2014;27:314-27.
50h. Nikiforov YE, Carty SE, Chiosea SI, Coyne C, Duvvuri U, Ferris RL, Gooding WE, LeBeau SO, Ohori NP, Seethala RR, Tublin ME, Yip L, Nikiforova MN. Impact of the Multi-Gene ThyroSeq Next-Generation Sequencing Assay on Cancer Diagnosis in Thyroid Nodules with Atypia of Undetermined Significance/Follicular Lesion of Undetermined Significance Cytology. Thyroid. 2015;25:1217-23.
- 51.
Durand S, Ferraro-Peyret C, Selmi-Ruby S, Paulin C, El Atifi M, Berger F, Berger-Dutrieux N, Decaussin M, Peix JL, Bournaud C, Orgiazzi J, Borson-Chazot F, Rousset B Evaluation of gene expression profiles in thyroid nodule biopsy material to diagnose thyroid cancer. J Clin Endocrinol Metab. 2008 Apr;93(4):1195-202.
51a. Mazeh H, Levy Y, Mizrahi I, Appelbaum L, Ilyayev N, Halle D, Freund HR, Nissan A. Differentiating benign from malignant thyroid nodules using micro ribonucleic acid amplification in residual cells obtained by fine needle aspiration biopsy. J Surg Res. 2013 Apr;180:216-21.
51b. Agretti P1, Ferrarini E, Rago T, Candelieri A, De Marco G, Dimida A, Niccolai F, Molinaro A, Di Coscio G, Pinchera A, Vitti P, Tonacchera M. MicroRNA expression profile helps to distinguish benign nodules from papillary thyroid carcinomas starting from cells of fine-needle aspiration. Eur J Endocrinol. 2012;167:393-400.
51c. Wei WJ, Shen CT, Song HJ, Qiu ZL, Luo QY. MicroRNAs as a potential tool in the differential diagnosis of thyroid cancer: a systematic review and meta-analysis. Clin Endocrinol (Oxf). 2014.
51d. Kitano M, Rahbari R, Patterson EE, Steinberg SM, Prasad NB, Wang Y, Zeiger MA, Kebebew E. Evaluation of candidate diagnostic microRNAs in thyroid fine-needle aspiration biopsy samples. Thyroid. 2012;22:285-91.
51e. Keutgen XM, Filicori F, Crowley MJ, Wang Y, Scognamiglio T, Hoda R, Buitrago D, Cooper D, Zeiger MA, Zarnegar R, Elemento O, Fahey TJ 3rd. A panel of four miRNAs accurately differentiates malignant from benign indeterminate thyroid lesions on fine needle aspiration. Clin Cancer Res. 2012;18(7):2032-8.
51f. Mazeh H, Mizrahi I, Halle D, Ilyayev N, Stojadinovic A, Trink B, Mitrani-Rosenbaum S, Roistacher M, Ariel I, Eid A, Freund HR, Nissan A. Development of a microRNA-based molecular assay for the detection of papillary thyroid carcinoma in aspiration biopsy samples. Thyroid. 2011;21(2):111-8.
51g. Kitano M1, Rahbari R, Patterson EE, Steinberg SM, Prasad NB, Wang Y, Zeiger MA, Kebebew E. Evaluation of candidate diagnostic microRNAs in thyroid fine-needle aspiration biopsy samples. Thyroid. 2012;22:285-91.
51h. Nishino M Molecular cytopathology for thyroid nodules: A review of methodology and test performance. Cancer Cytopathol. 2016 Jan;124(1):14-27. doi: 10.1002/cncy.21612. Epub 2015 Sep 8.
51i. Gharib H, Papini E, Garber JR, Duick DS, Harrell RM, Hegedüs L, Paschke R, Valcavi R, Vitti P; American Association Of Clinical Endocrinologists, American College Of Endocrinology, And Associazione Medici Endocrinologi Medical Guidelines For Clinical Practice For The Diagnosis And Management Of Thyroid Nodules - 2016 UPDATE. Endocr Pract. 2016 May;22(5):622-39. doi: 10.4158/EP161208.GL.
52 Clark, O, Okerlund, M, Cavalieri, R, Greenspan, F 1979. Diagnosis and treatment of thyroid; parathyroid; and thyroglossal duct cysts. J Clin Endocrinol Metab 48:983
52.1 Leboulleux S, Girard E, Rose M, Travagli JP, Sabbah N, Caillou B, Hartl DM, Lassau N, Baudin E, Schlumberger M Ultrasound criteria of malignancy for cervical lymph nodes in patients followed up for differentiated thyroid cancer. J Clin Endocrinol Metab. 2007 Sep;92(9):3590-4
53. Marcocci, C, Vitti, P, Cetani, F, Catalano, F, Concetti, R, Pinchera, A 1991. Thyroid ultrasonography helps to identify patients with diffuse lymphocytic thyroiditis who are prone to develop hypothyroidism. J Clin Endocrinol Metab 72:209-13
54. Kendall, L, Condon, R 1969. Prediction of malignancy in solitary thyroid nodules. Lancet 1:1071
55. Miller, J, Hamburger, J 1965.. The thyroid scintigram. 1. The hot nodule. Radiology 84:66
56. Attie, J 1960. The use of radioactive iodine in the evaluation of thyroid nodules. Surgery 47:611
57. Dische, S 1964. The radioisotope scan applied to the detection of carcinoma in thyroid swellings. Cancer 17:473
58. Fujimoto, Y, Oka, A, Nagataki, S 1972. Occurrence of papillary carcinoma in hyperfunctioning thyroid nodule. Report of a case. Endocrinol Jpn 19:371
59. Scott, M, Crawford, J 1976. Solitary thyroid nodules in childhood. Is the incidence of thyroid carcinoma declining? Pediatrics 58:521
60.Messaris, G, Evangelou, G, Tountas, C 1973. Incidence of carcinoma in cold nodules of the thyroid gland. Surgery 74:447
61. Van den Bruel, A, Maes, A, De Potter, T, et al. 2002 Clinical relevance of thyroid fluorodeoxyglucose-whole body positron emission tomography incidentaloma. J Clin Endocrinol Metab 87:1517-20
62. Hakama, M Berlin; Springer-Verlag Different world thyroid cancer rates; in Hedinger CE (ed). Thyroid Cancer. International Union Against Cancer Monograph Series:Vol 12.
63. Young, J J, Percy, C, Asire, A e 1082 pages Surveillance; Epidemiology; and End Results. Incidence and Mortality Data; 1973-77. National Cancer Institute Monograph 57 NIH Publication No. 81:2330
64. Goldstein, R, Hart, I 1983. Follow-up of solitary autonomous thyroid nodules treated with 131I. New Engl J Med 309:1473
65. Gorman, C, Robertson, J 1978. Radiation dose in the selection of 131I or surgical treatment for toxic thyroid adenoma. Ann Intern Med 89:85
66. Paracchi, A, Ferrari, C, Livraghi, T, et al. 1992. Percutaneous intranodular ethanol injection. A new treatment for autonomous thyroid adenoma. J Endocrinol Invest 15:353-362
67. Lippi, F, Ferrari, C, Manetti, L, et al. 1996. Treatment of solitary autonomous thyroid nodules by percutaneous ethanol injection. results of an Italian multicenter study. The Multicenter Study Group. J Clin Endocrinol Metab 81:3261-3264
68. Monzani, F, Caraccio, N, Goletti, O, et al. S54-8 Treatment of hyperfunctioning thyroid nodules with percutaneous ethanol injection. Eight years' experience. Exp Clin Endocrinol Diabetes 106: Suppl 4
69. Hamburger, J I 1980; Evolution of toxicity in solitary nontoxic autonomously functioning thyroid nodules. J Clin Endocrinol Metab 50:1089-1093
70. McCowen, K, Reed, J, BL., F 1980. The role of thyroid therapy in patients with thyroid cysts. Amer J Med 68:853
71. Treece, G, Georgitis, W, Hofeldt, F 1983 Resolution of recurrent thyroid cysts with tetracycline instillation. Arch Int Med 143: 2285.
72. Monzani, F, Lippi, F, Goletti, O, et al. 1994. Percutaneous aspiration and ethanol sclero-therapy for thyroid cysts. J Clin Endocrinol Metab 78:800-802
73. Zingrillo, M, Torlontano, M, Ghiggi, M, et al. 1996. Percutaneous ethanol injection of large thyroid cystic nodules. Thyroid 6:403-8
74.Del Prete, S, Caraglia, M, Russo, D, et al. 2002 Percutaneous ethanol injection efficacy in the treatment of large symptomatic thyroid cystic nodules: ten-year follow-up of a large series. Thyroid 12:815-21
75. see 70
76. Papini, E, Bacci, V, Panunzi, C, et al. 1993. A prospective randomized trial of levothyroxine suppressive therapy for solitary thyroid nodules. Clin Endocrinol 38:507-513
77. Burch, H 1995. Evaluation and management of the solid thyroid nodule. Endocrinol Metab Clin N Am 24:663-710
78. Mainini, E, Martinelli, I, Morandi, G, Villa, S, Stefani, I, Mazzi, C 1995. Levothyroxine suppressive therapy for solitary thyroid nodule. J Endocrinol Invest 18:796-799
79. Cooper, D 1995. Clinical review 66. Thyroxine suppression therapy for benign nodular disease. J Clin Endocrinol Metab 80:331-334
80. Castro, M R, Caraballo, P J, Morris, J C 2002 Effectiveness of thyroid hormone suppressive therapy in benign solitary thyroid nodules: a meta-analysis. J Clin Endocrinol Metab 87:4154-9
81 Zelmanovits, F, Genro, S, Gross, J 1998. Suppressive therapy with levothyroxine for solitary thyroid nodules. A double-blind controlled clinical study and cumulative meta-analyses. J Clin Endocrinol Metab 83:3881-3885
82. Herms, A, Huysmans, D 1998. Treatment of benign nodular thyroid disease. N Engl J Med 312:601-4
83. Larosa, G, Ippolito, A, Luppo, L, et al. 1996. Cold thyroid nodule reduction with l-thyroxine can be predicted by initial nodule volume and cytological characteristics. J Clin Endocrinol Metab; 81:4385-7
83.a. Sdano MT, Falciglia M, Welge JA, Steward DL. Efficacy of thyroid hormone suppression for benign thyroid nodules: meta-analysis of randomized trials Otolaryngol Head Neck Surg. 2005 Sep;133(3):391-6
84. Wemeau, J L, Caron, P, Schvartz, C, et al. 2002 Effects of thyroid-stimulating hormone suppression with levothyroxine in reducing the volume of solitary thyroid nodules and improving extranodular nonpalpable changes: a randomized, double-blind, placebo-controlled trial by the French Thyroid Research Group. J Clin Endocrinol Metab 87:4928-34
85 see 77
86 Morita, T, Tamai, H, Ohshima, A, et al. 1989. Changes in serum thyroid hormone; thyrotropin and thyroglobulin concentrations during thyroxine therapy in patients with solitary thyroid nodules. J Clin Endocrinol Metab 69:227
87 Woolner, L, Beahrs, O, Black, B, McConahey, W, Keating, F J vol 12 Long term survival rates. in Hedinger Chr E (ed). Thyroid Cancer. International Union Against Cancer: Monograph Series
88. Fogelfeld, L, Wiviott, M, Shore-Freedman, E, et al. 1989. Recurrence of thyroid nodules after surgical removal in patients irradiated in childhood for benign conditions. N Engl J Med 320:835-840
89. Bennedbaek, F, Hegedus, L 1999. Percutaneous ethanol injection therapy in benign solitary solid cold thyroid nodules. A randomized trial comparing one injection with three injections. Thyroid 9:225-233
89.1 Døssing H, Bennedbæk FN, Hegedüs L. Long-term outcome following interstitial laser photocoagulation of benign cold thyroid nodules. Eur J Endocrinol. 2011 Jul;165(1):123-8.
90. Khurana, K, Labrador, E, Izquierdo, R, Mesonero, C, Pisharodi, L 1999. The role of fine-needle aspiration biopsy in the management of thyroid nodules in children; adolescents; and young adults. A multi-institutional study. Thyroid 9:383
91.Tan, G, Gharib, H 1997. Thyroid incidentalomas. management approaches to nonpalpable nodules discovered incidentally on thyroid imaging. Ann Intern Med 126:226-31
- ABSTRACT
- INTRODUCTION
- DEFINITION
- PATHOLOGY OF NODULES
- CAUSE OF NODULES
- COURSE AND SYMPTOMS OF NODULES
- HOT NODULES
- METABOLIC FUNCTION OF NODULES
- CLINICAL EVALUATION AND MANAGEMENT OF NODULES
- HISTORY OF NODULES
- PHYSICAL FINDINGS
- FINE NEEDLE ASPIRATION CYTOLOGY
- GENETIC DIAGNOSIS
- THYROID ULTRASOUND
- ISOTOPE SCANS
- THE DECISION FOR SURGERY
- THYROXINE TREATMENT
- SCLEROTHERAPY
- THYROID NODULES IN CHILDREN
- INCIDENTALOMAS
- REFERENCES
- Utility of fine-needle aspiration cytology and frozen-section examination in the operative management of thyroid nodules.[Am Surg. 1997]Utility of fine-needle aspiration cytology and frozen-section examination in the operative management of thyroid nodules.Davoudi MM, Yeh KA, Wei JP. Am Surg. 1997 Dec; 63(12):1084-9; discussion 1089-90.
- Fine-needle aspiration biopsy of the thyroid: comparison between thyroid palpation and ultrasonography.[Endocr Pract. 2002]Fine-needle aspiration biopsy of the thyroid: comparison between thyroid palpation and ultrasonography.Deandrea M, Mormile A, Veglio M, Motta M, Pellerito R, Gallone G, Grassi A, Torchio B, Bradac R, Garberoglio R, et al. Endocr Pract. 2002 Jul-Aug; 8(4):282-6.
- One in four patients with follicular thyroid cytology (THY3) has a thyroid carcinoma.[Thyroid. 2009]One in four patients with follicular thyroid cytology (THY3) has a thyroid carcinoma.Mihai R, Parker AJ, Roskell D, Sadler GP. Thyroid. 2009 Jan; 19(1):33-7.
- Review [Thyroid nodules: benign or malignant?].[Rev Med Brux. 2011]Review [Thyroid nodules: benign or malignant?].Liénart F, Charret F, Daper C, Dekeyser C, Ducobu J, Malengreau A, Van Coevorden A. Rev Med Brux. 2011 Sep-Oct; 32(5):445-52.
- Review [Thyroid nodule: benign or malignant?].[Rev Med Brux. 2012]Review [Thyroid nodule: benign or malignant?].Liénart F. Rev Med Brux. 2012 Sep; 33(4):254-62.
- Thyroid Nodules - EndotextThyroid Nodules - Endotext
- PTPRC protein tyrosine phosphatase receptor type C [Homo sapiens]PTPRC protein tyrosine phosphatase receptor type C [Homo sapiens]Gene ID:5788Gene
- 5788[uid] AND (alive[prop]) (1)Gene
- TALAM1 TALAM1 transcript, MALAT1 antisense RNA [Homo sapiens]TALAM1 TALAM1 transcript, MALAT1 antisense RNA [Homo sapiens]Gene ID:109136579Gene
- RAB30-DT RAB30 divergent transcript [Homo sapiens]RAB30-DT RAB30 divergent transcript [Homo sapiens]Gene ID:100506233Gene
Your browsing activity is empty.
Activity recording is turned off.
See more...