

NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-.

ABSTRACT
The major cause of hypoglycemia is iatrogenic. Treatment with an insulin secretagogue, including sulfonylureas or glinides, or insulin, particularly when coupled with compromised defenses against the resulting falling plasma glucose concentrations, is the limiting factor in the glycemic management of diabetes. It causes recurrent morbidity in most people with type 1 diabetes mellitus (T1DM) and many with advanced type 2 diabetes mellitus (T2DM) and is sometimes fatal. Low blood glucose also impairs physiological and behavioral defenses against subsequent hypoglycemia, further increasing the risk of hypoglycemia and its complications including adverse cardiovascular effects. Strategies to reduce hypoglycemia are based on the individual’s age, regimen, and comorbidities. A patient-centered approach, newer insulin analogues, novel insulin delivery devices, and continuous glucose monitoring help reduce the risk of hypoglycemia and optimize glycemia. For complete coverage of all related areas of Endocrinology, please visit our on-line FREE web-text, WWW.ENDOTEXT.ORG.
THE CLINICAL PROBLEM OF HYPOGLYCEMIA IN DIABETES
The problem of iatrogenic hypoglycemia in diabetes has been reviewed in detail (1–6).
Glycemic Control
In the context of comprehensive treatment, including weight, blood pressure, and blood lipid control among other measures, normoglycemia makes a difference for people with diabetes. Improved glycemic control reduces microvascular complications (retinopathy, nephropathy, and neuropathy) in both type 1 diabetes mellitus (T1DM) (7) and type 2 diabetes mellitus (T2DM) (8,9). Follow-up of patients with T1DM (10) and T2DM (11) suggests that an improved earlier period of glycemic control may also reduce subsequent macrovascular complications. Thus, safe and long-term maintenance of physiologic normoglycemia is in the best interest of people with diabetes.
The Limiting Factor
Iatrogenic hypoglycemia, fundamentally but not exclusively usually results from treatment with an insulin secretagogue or insulin either alone or in combination with other glucose lowering medications, and is the major limiting factor in the goal of near normoglycemia in the management of diabetes (1). Iatrogenic hypoglycemia causes recurrent morbidity in most people with T1DM and many with advanced T2DM and is sometimes fatal (4). It impairs defenses against subsequent falling plasma glucose concentrations and results in a vicious cycle of recurrent hypoglycemia. It generally precludes maintenance of euglycemia over a lifetime of diabetes and, thus, full realization of the benefits of glycemic control.
Type 1 and Type 2 Diabetes
Iatrogenic hypoglycemia commonly occurs in the overwhelming majority of people with T1DM who must, of course, be treated with insulin. Most have untold numbers of episodes of asymptomatic hypoglycemia. These are not benign since they impair defenses against subsequent hypoglycemia (1). Individuals with T1DM suffer an average of two episodes of symptomatic hypoglycemia per week – thousands of such episodes over a lifetime of diabetes – and about one episode of disabling severe (i.e., requiring assistance) hypoglycemia per year. Hypoglycemia causes brain fuel deprivation that, if unchecked, results in functional brain failure that is typically corrected after the plasma glucose concentration is raised (12). Rarely, if low blood glucose is profound and prolonged, it can result in brain death (12). Hypoglycemia may lead to cardiac arrhythmias, especially in patients with preexisting cardiac abnormalities (13,14). Additionally, hypoglycemia has been demonstrated to be pro-coagulant and pro-atherothrombotic (15,16). Furthermore, severe hypoglycemia has been associated with increased risk of death extending many months and up to one year after the sentinel episode (17). Of concern, roughly from 2 to 10 percent of deaths of people with diabetes were the result of hypoglycemia (4,5,14,18,19). Regardless of the actual rate, the fact that there is an iatrogenic hypoglycemia mortality rate is alarming.
Overall, for a given individual, iatrogenic hypoglycemia is less frequent in T2DM (1,20,21). However, due to the greatly increased numbers of individuals with T2DM, the prevalence of hypoglycemic episodes is actually greater than in T1DM. Drugs that can cause endogenous or exogenous (insulin) hyperinsulinemia unregulated by glucose can cause hypoglycemia. On the other hand, insulin sensitizers (metformin or a thiazolidinedione), α-glucosidase inhibitors, sodium glucose cotransporter 2 inhibitors, and drugs such as dipeptidyl peptidase-IV inhibitors and glucagon-like peptide-1 receptor agonists (GLP-1 RAs) that cause glucose-dependent hyperinsulinemia should not, and probably do not, cause hypoglycemia. They do, however, increase the risk of hypoglycemia if used with an insulin secretagogue or with insulin. Even during treatment of T2DM with insulin, hypoglycemia event rates are about one-third of those in T1DM overall (20). However, for reasons discussed shortly (see Glucose Counterregulatory Physiology and its Pathophysiology in Diabetes), the incidence of iatrogenic hypoglycemia increases over time, approaching that in T1DM, as people approach the insulin deficient end of the spectrum of T2DM (21). Because T2DM is roughly 20-fold more prevalent than T1DM and many, perhaps most, people with T2DM ultimately require treatment with insulin, most episodes of hypoglycemia, including those of severe hypoglycemia, occur in individuals with T2DM. Insulin secretagogue and insulin induced hypoglycemia can be fatal in T2DM although precise hypoglycemic mortality rates are as yet known. As many as 10% of patients with severe sulfonylurea-induced hypoglycemia die (22).
DEFINITION AND CLASSIFICATION OF HYPOGLYCEMIA
The American Diabetes Association and the International Hypoglycemia Study Group (Table 1) define clinically significant hypoglycemia as a blood glucose <54 mg/dl (3.0 mmol/L) which is detected by the individual’s self-monitoring blood glucose (SMBG) as well as by continuous glucose monitoring ((CGM), glucose values of <54 mg/dl (3.0 mmol/L) for at least 20 min), or laboratory measurement of plasma glucose which is sufficiently low to indicate clinically significant hypoglycemia (23,24). Blood glucose ≤70 mg/dl (3.9 mmol/L) is considered a hypoglycemia alert value, which represents an important lower glucose cutoff value for treatment with fast-acting carbohydrates and dose adjustments of antidiabetic medications. Severe hypoglycemia is defined as a low glucose value with severe cognitive impairment that requires assistance from another person in order to achieve recovery (25). Relative hypoglycemia or pseudohypoglycemia represents an event during which the person with diabetes reports any of the typical symptoms of hypoglycemia and interprets those as indicative of hypoglycemia with a measured plasma glucose concentration >70 mg/dL (>3.9 mmol/L).
Table 1.
| Level | Glycemic criteria | |
|---|---|---|
| Hypoglycemia alert value | ≤70 mg/dl (3.9 mmol/L) | Sufficiently low for treatment with fast |
| (level 1) | acting carbohydrate and dose adjustment | |
| of glucose lowering therapy | ||
| Clinically significant hypoglycemia (level 2) | <54 mg/dl (3.0 mmol/L) | Sufficiently low to indicate serious, clinically important hypoglycemia |
| Severe hypoglycemia (level 3) | No specific glucose threshold | Hypoglycemia associated with severe cognitive impairment requiring external assistance for recovery |
COMPLICATIONS OF HYPOGLYCEMIA
Increased mortality has been observed in randomized controlled trials during more aggressive compared with less aggressive glucose-lowering therapy in patients with T2DM (26) and in patients with hypoglycemia in intensive care units (27). In addition, intensive glycemic control has not been shown to improve cardiovascular outcomes in patients with T2DM (28). The associations between increased hypoglycemia and increased morbidity and mortality during aggressive glycemic therapy in these and other (18,29,30) trials have been thought to be multifactorial (31). A possible explanation is that aggressive reduction of blood glucose increases the risk of hypoglycemia. The latter can trigger sympathoadrenal activation with the release of catecholamines, cause abnormal cardiac repolarization, and lead to myocardial ischemia. Hypoglycemia-induced ECG changes include ST-segment depression, atrial and ventricular ectopic beats, P- and T-wave abnormalities, and QT-interval prolongation (32). Low blood glucose creates procoagulant and prothrombotic states and induces inflammation and oxidative stress (33,34).
The association of hypoglycemia with cognitive function appears to be more complicated. Among older individuals with type 2 diabetes, a history of severe hypoglycemia was associated with a greater risk of dementia (37). The ACCORD study reported that cognitive impairment at baseline and a continuing decline in cognitive function among individuals were associated with a greater risk for dementia following hypoglycemia (35). It should be noted however that in DCCT/EDIC, which involved much younger participants, no association of severe hypoglycemia and cognitive decline was found (25, 39).
Hypoglycemic episodes can create fear of subsequent hypoglycemia and negatively affect the quality of life in T1DM as well as T2DM (36). Some of the consequences may include anxiety, shortness of breath, palpitations, tremors, symptoms of depression, and reduced ability to function.
GLUCOSE COUNTERREGULATORY PHYSIOLOGY AND ITS PATHOPHYSIOLOGY IN DIABETES
Physiology
In nondiabetic individuals, there are a number of physiological defenses against falling plasma glucose concentrations. These include reductions in insulin secretion, which occur as glucose levels decline within the physiological range. This allows for increased hepatic (and renal) glucose production, and increments in glucagon and epinephrine secretion, which occur as glucose levels fall just below the physiological range and stimulate hepatic glucose production (1,2,37) (Figure 1). Increased epinephrine levels also normally mobilize gluconeogenic precursors from muscle and fat, stimulate renal glucose production, limit glucose utilization by muscle and fat, and limit insulin secretion (2). The behavioral defense against falling plasma glucose concentrations is carbohydrate ingestion prompted largely by the perception of neurogenic (autonomic) symptoms (e.g., palpitations, tremor, and anxiety/arousal which are catecholamine-mediated or adrenergic and sweating, hunger, and paresthesias which are sympatho-adrenal mediated or cholinergic) (38,39) (Figure 1). These are largely sympathetic neural, rather than adrenomedullary, in origin (39). The extent to which mild neuroglycopenic symptoms such as altered mentation or psychomotor changes contribute to the patient’s recognition of hypoglycemia is unclear; awareness of hypoglycemia is largely prevented by pharmacological antagonism of neurogenic symptoms (38). Severe neuroglycopenic symptoms include frank confusion, acute focal or central neurologic deficits, seizure and/or loss of consciousness. All of these defenses can be compromised in T1DM and advanced T2DM (1,40,41).
Pathophysiology
Episodes of therapeutic hyperinsulinemia, the result of glucose unregulated delivery of endogenous (insulin secretagogue therapy) or exogenous (insulin therapy) insulin into the circulation, initiate the sequence that may, or may not, culminate in an episode of hypoglycemia (1). Absolute therapeutic insulin excess of sufficient magnitude can cause isolated episodes of hypoglycemia despite intact glucose counterregulatory defenses against hypoglycemia (Figure 2). But that is an uncommon event. Iatrogenic hypoglycemia is typically the result of the interplay of mild-moderate absolute therapeutic insulin excess, reduced glucose intake, exercise, increased insulin sensitivity, sleep, and existing or induced compromised physiological and behavioral defenses against falling plasma glucose concentrations in T1DM (1,40) and T2DM (1,41). In T1DM, because of β-cell failure, insulin levels do not decrease as glucose levels fall; the first physiological defense is lost. Furthermore, glucagon levels do not increase as glucose levels fall (42); the second physiological defense is lost. That, too, is possibly attributable to a β-cell signaling failure since a decrease in β-cell secretion, coupled with a low α-cell glucose concentration, normally signals α-cell glucagon secretion (3,43,44). Finally, the increase in epinephrine levels as glucose levels fall is also attenuated ((1,41); and thus, the three major physiological defenses are compromised.
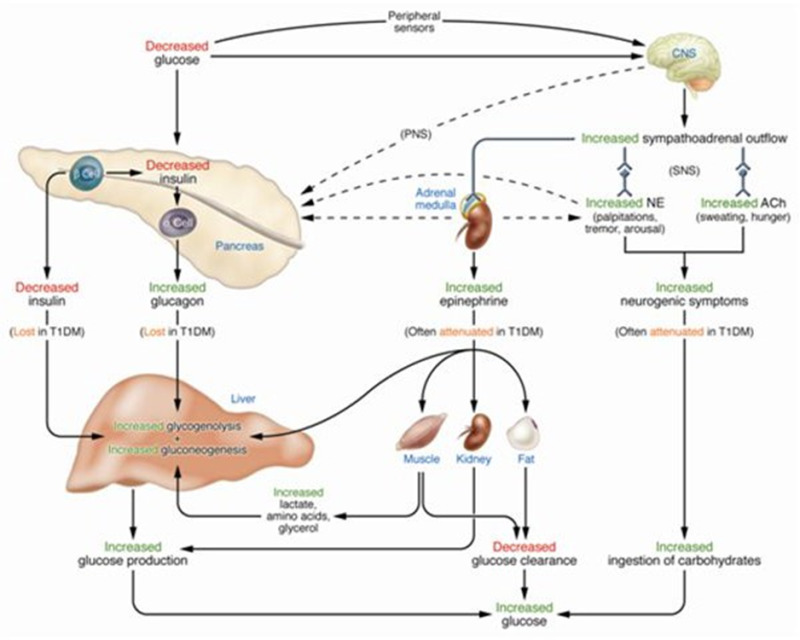
Figure 1.
Physiological and Behavioral Defenses Against Hypoglycemia in Humans. ACH, acetylcholine; NE, norepinephrine; PNS, parasympathetic nervous system; SNS, sympathetic nervous system. From reference (45).
Although it is often caused by recent antecedent hypoglycemia (40,46) or by prior exercise (47) or sleep (48–50), the mechanism of the attenuated sympathoadrenal response to falling glucose levels is unknown (3). Nonetheless, the attenuated epinephrine response is a marker of an attenuated sympathetic neural response (39) and the latter largely results in the reduction of the symptoms of hypoglycemia causing hypoglycemia unawareness (or impaired awareness of hypoglycemia) and thus loss of the behavioral defense, i.e., carbohydrate ingestion. In the setting of therapeutic hyperinsulinemia, falling plasma glucose concentrations, absent decrements in insulin, absent increments in glucagon, and attenuated increases in epinephrine cause the clinical syndrome of defective glucose counter-regulation (1,40), which is associated with a 25-fold (51) or greater (52) increased risk of iatrogenic hypoglycemia. The attenuated sympathoadrenal, particularly the attenuated sympathetic neural response, causes the clinical syndrome of hypoglycemia unawareness (1) which is associated with a 6-fold increased risk of iatrogenic hypoglycemia (53).
The pathophysiology of glucose counter-regulation is the same in T1DM and T2DM albeit with different time courses. β-cell failure, and therefore loss of the insulin and glucagon responses to falling plasma glucose concentrations, develops early in T1DM but more gradually in T2DM. Thus, iatrogenic hypoglycemia, becomes a common problem early in T1DM and later in T2DM.
The concept of hypoglycemia-associated autonomic failure (HAAF) in diabetes (1,3,5,40,41) (Figure 2) posits that recent antecedent hypoglycemia, as well as prior moderate exercise or sleep, causes both defective glucose counter-regulation (by reducing increments in epinephrine in the setting of absent decrements in insulin and absent increments in glucagon during subsequent hypoglycemia) and hypoglycemia unawareness (by reducing sympathoadrenal and resulting neurogenic symptom responses during subsequent hypoglycemia) and, therefore, a vicious cycle of recurrent hypoglycemia. Supporting this concept is the finding, that as little as 2-3 weeks of scrupulous avoidance of hypoglycemia reverses hypoglycemia unawareness and improves the attenuated epinephrine component of defective glucose counter-regulation in most affected patients. (54–57).
The mechanism(s) of the attenuated sympathoadrenal response to falling glucose levels, the key feature of HAAF, is not known (3). It must involve the central nervous system or the afferent or efferent components of the sympathoadrenal system. Theories include increased blood-to-brain transport of a metabolic fuel, effects of a systemic mediator such as cortisol on the brain, altered hypothalamic mechanisms, and activation of an inhibitory cerebral network mediated through the thalamus (3).

RISK FACTORS FOR HYPOGLYCEMIA IN DIABETES
Conventional Risk Factors
The conventional risk factors are based on the premise that relative to low rates of glucose delivery into the circulation, high rates of glucose efflux out of the circulation, or both, or absolute therapeutic hyperinsulinemia is the sole determinant of risk (1). They include (but are not limited to):
- 1.
Insulin (or insulin secretagogue) doses are excessive, ill-timed, or of the wrong type.
- 2.
Exogenous glucose delivery is decreased (as following missed meals and during the overnight fast, with gastroparesis or celiac disease).
- 3.
Glucose utilization and sensitivity to insulin are increased (as during and shortly after exercise, in the middle of the night, following weight loss, or improved glycemic control).
- 4.
Endogenous glucose production is decreased (as following alcohol ingestion or in liver failure).
- 5.
Insulin clearance is decreased (as in renal failure).
- 6.
Classical diabetic autonomic neuropathy.
Patients with diabetes and their caregivers must consider each of these risk factors carefully whenever hypoglycemia is a problem (58).
Risk Factors Indicative of Hypoglycemia-Associated Autonomic Failure (HAAF)
These risk factors stem directly from the pathophysiology of glucose counter-regulation and the concept of HAAF in diabetes (1,40,41). They include:
- 1.
The degree of absolute endogenous insulin deficiency. This determines the extent to which insulin levels will not decrease and glucagon levels will not increase as plasma glucose concentrations fall in response to therapeutic hyperinsulinemia. It is in part a function of the duration of diabetes.
- 2.
A history of severe hypoglycemia, hypoglycemia unawareness, or both as well as recent antecedent hypoglycemia, prior exercise or sleep.
- 3.
Aggressive glycemic therapy per se (lower A1C levels, lower glycemic goals). Studies with a control group treated to higher mean glycemia consistently document higher rates of hypoglycemia in individuals treated to lower mean glycemia (e.g. (4)). Mean glycemia is a risk factor for hypoglycemia. However, severe hypoglycemia can occur in individuals with any A1C level, and the fact that mean glycemia is a risk factor does not mean that one cannot both lower mean glycemia and reduce the risk of hypoglycemia in individual patients (6).
PREVENTION OF HYPOGLYCEMIA IN DIABETES
The prevention of hypoglycemia can be viewed as a process with four steps (1,6). The first step is acknowledging the problem; the second - considering the conventional risk factors in diabetes; the third – considering the risk factors indicative of HAAF in diabetes; and the fourth - application of the relevant principles of intensive glycemic therapy of diabetes.
Acknowledge the Problem
The issue of hypoglycemia should be addressed at every contact with a patient treated with an insulin secretagogue or with insulin (6). In addition to the patient’s comments and review of the individual’s SMBG data (as well as any CGM data) we find it especially helpful to inquire what is the glucose level when each patient can detect hypoglycemia and what are the symptoms and signs at various hypoglycemic levels. It is also often helpful to question close associates of the patient since they may have observed clues to episodes of hypoglycemia. Patient concerns about the reality, or even the possibility, of hypoglycemia can be a barrier to glycemic control (59,60). Their concerns need to be discussed and addressed if hypoglycemia is a real or perceived problem.
Consider the Conventional Risk Factors for Hypoglycemia in Diabetes
Each of the risk factors that result in relative or absolute therapeutic hyperinsulinemia, as just discussed, should be considered carefully in any patient with iatrogenic hypoglycemia. Those include the dose, timing, and type of the insulin secretagogue or insulin preparations(s) used, and conditions in which exogenous glucose delivery or endogenous glucose production is decreased, glucose utilization or insulin sensitivity is increased or insulin clearance is decreased.
Consider the Risk Factors Indicative of HAAF in Diabetes
As detailed earlier, the risk factors indicative of HAAF include the degree of absolute endogenous insulin deficiency, a history of severe hypoglycemia, impaired awareness of hypoglycemia, or both as well as any relationship between iatrogenic hypoglycemia and recent antecedent hypoglycemia, prior exercise or sleep, and lower glycemic goals. A history of severe hypoglycemia is a clinical red flag. Without a fundamental adjustment of the treatment regimen, the likelihood of another episode is high (7,61).
Apply the Relevant Principles of Intensive Glycemic Therapy
The principles of intensive glycemic therapy relevant to minimizing the risk of iatrogenic hypoglycemia in diabetes include drug selection, selective application of diabetes treatment technologies, individualized glycemic goals, structured patient education, and short-term scrupulous avoidance of hypoglycemia (6). Based on the premise that the risk of hypoglycemia is modifiable, the International Hypoglycemia Study Group recommended that people with diabetes treated with a sulfonylurea, a glinide, or insulin should be educated about hypoglycemia, should treat self- monitored plasma glucose (SMPG) <70 mg/dL (<3.9 mmol/L) to avoid progression to clinical iatrogenic hypoglycemia, and should regularly be queried about hypoglycemia, including the glucose level at which symptoms develop (6).
Drug selection relevant to minimizing the risk of hypoglycemia includes avoidance, if possible, of sulfonylureas or glinides, the use of more physiological insulin regimens (62), and the use of long-acting or even ultra-long-acting daily basal insulin analogues and rapid-acting prandial insulin analogues in lieu of human insulins (63–66). Insulin analogues reduce the frequency of at least nocturnal hypoglycemia (63–65) including severe nocturnal hypoglycemia (65) compared to human insulins. In insulin-requiring T2DM, basal insulins are associated with less hypoglycemia than prandial insulin regimens. Furthermore, the combination of a long-acting basal insulin with a glucose-lowering drug with low hypoglycemic potential (e.g., a GLP-1 receptor agonist) may result in less hypoglycemia than with the use of basal-bolus insulin therapy (67).
Relevant diabetes treatment technologies include continuous subcutaneous insulin infusion (CSII), continuous glucose monitoring (CGM), and combinations of CSII and CGM. Although earlier meta-analyses disclosed little (68) or no (69) advantage of CSII, recent evidence suggest that CSII treatment is superior in achieving glucose control compared to multiple daily injections (70,71). CGM devices alone have been shown to improve glycemic control and decrease duration of hypoglycemia in patients with diabetes mellitus (72,73). As their accuracy is continuously improving, several CGM systems have been approved by the FDA, and other regulatory authorities to even replace point of care blood glucose testing (74,75). Real-time CGM systems have also been found to improve hypoglycemia awareness, without a change in A1C, in a small group of patients with T1DM (76). A favorable experience with CSII has also been reported (77,78). The combination of CSII and real-time CGM – sensor augmented pump therapy, particularly that including an insulin pump programmed to stop insulin infusion for up to two hours when CGM values fall to a selected glucose level (“low glucose suspend”) – has been reported to reduce the frequency of severe hypoglycemia in T1DM (79–81). Recent innovations have included cessation of insulin delivery during hypoglycemia. Several promising studies have investigated approaches for leading closed-loop insulin (or insulin and glucagon) replacement. The development of automated closed-loop insulin pumps represents an area of ongoing research and fully closed-loop insulin (82) or insulin and glucagon replacement (83) and pancreatic islet transplantation (84) will undoubtedly eliminate hypoglycemia and improve overall glycemic control. A hybrid-not fully automated -system (as only basal insulin is automatically adjusted) has received approval by the FDA (85).
Special circumstances relevant to drug selection and treatment technologies in the prevention of hypoglycemia in diabetes include exercise, the overnight period, the elderly, drivers, and pregnancy. Especially in insulin-treated patients’ hypoglycemia can occur during or shortly after exercise (86) or late after exercise (87,88). Measures to avoid early-onset exercise hypoglycemia include interspersing episodes of intense exercise (which tends to raise plasma glucose concentrations), adding carbohydrate ingestion, and reducing insulin doses (89). A consistent observation since the DCCT (7) is that more than half of episodes of hypoglycemia, including severe hypoglycemia, occur during the night. That is typically the longest interval between meals and between SMPG and includes the time of maximal sensitivity to insulin. In addition to the use of insulin analogues, sensor augmented pump therapy or closed-loop insulin or insulin and glucagon replacement, all discussed earlier, approaches to the prevention of nocturnal hypoglycemia include attempts to produce sustained delivery of exogenous carbohydrate or sustained endogenous glucose production (90). With respect to the former approach, a conventional bedtime snack or bedtime administration of uncooked cornstarch have not been found to be consistently effective (90). With respect to the latter approach an experimental treatment is bedtime administration of a β2-adrenergic agonist such as terbutaline (90–92). In addition to HAAF, comorbidities including renal insufficiency, polypharmacy, and impaired cognition are more relevant to the development of hypoglycemia in older individuals (93). Drivers with diabetes and a history of recurrent hypoglycemia-related driving mishaps have been found to have greater driving simulator impairments (94). Finally, up to 45% of pregnant women with type 1 diabetes experience severe hypoglycemia especially in the first trimester (95).
Individualized Glycemic Goal
Glycemic goals should be individualized in patients with diabetes (4,96). The selection of a glycemic goal in a person with diabetes is a trade-off between the benefits of glycemic control – partial prevention or delay of microvascular complications – and the risk of recurrent morbidity, and potential mortality, of hypoglycemia (4). A reasonable individualized glycemic goal is the lowest A1C that does not cause severe hypoglycemia and preserves awareness of hypoglycemia, preferably with little or no symptomatic or even asymptomatic hypoglycemia, at a given stage in the evolution of the individual’s diabetes (4). Thus, the glycemic goal should be linked not only to the level of glycemic control (i.e., the A1C) but also to the risk of hypoglycemia, specifically the drugs used (a sulfonylurea, a glinide, or insulin), the degree of endogenous insulin deficiency, and the anticipated benefit of the targeted level of glycemic control. A nondiabetic A1C would be reasonable in a patient with early T2DM treated effectively with lifestyle changes and/or drugs that do not cause hypoglycemia. For the majority of non-pregnant adults, a reasonable goal for an A1C is <7% (53 mmol/mol). For selected individuals with long life expectancy, without significant comorbidities (especially cardiovascular disease), stringent A1c goals (<6.5% (48 mmol/mol)) should be targeted, if this can be achieved without significant hypoglycemia (23). For children and adolescents, an A1C of <7.5% (58 mmol/mol) should be the goal, although a lower target (<7% (53 mmol/mol)) should be reasonable if it can be achieved without excessive hypoglycemia (97). However much higher levels of A1C (7.5%-8.0% (58-64 mmol/mol)) may be appropriate in elderly patients where hypoglycemia may be harmful. Even higher targets (A1C<8.5% (69 mmol/mol)) may be appropriate in individuals with very limited life expectancy (93).
Of note, it needs to be underscored that severe hypoglycemia can and does occur at A1C levels between 8-10% (64-86 mmol/mol) or higher in either T1DM or T2DM. Thus, severe hypoglycemia is not just a consequence of “low or near normal” A1C values. Of concern are recent data that severe hypoglycemia occurring in T2DM individuals >60 years with elevated A1C may have greater serious adverse events and increased mortality compared to individuals with improved glycemic control and lower A1C values.
Thus, attempts to improve glycemic control with insulin in T2DM individuals that have been resistant or proven challenging to strategies to lower glucose levels may be at greater risk for severe hypoglycemia and associated serious adverse events (18,26,29,30).
Structured Patient Education
The core approach, applicable to virtually all patients with diabetes treated with a sulfonylurea, a glinide, or insulin in whom hypoglycemia becomes a problem, is thorough, structured patient education (often re- education) that teaches the patient how and when their drugs can cause hypoglycemia, how to adjust their medications, meal plans, and exercise to optimize glycemic control and minimize hypoglycemia, and how to recognize and treat hypoglycemia (6). Based conceptually on earlier inpatient education programs (98), there is increasing evidence that outpatient structured education programs decrease hypoglycemia, often with a decrease in A1C (99–103). For example, a structured patient education program in flexible insulin therapy led to a reduction of impaired awareness of hypoglycemia (45% of those with impaired awareness initially were aware at one year) and a reduction in severe hypoglycemia (from 1.9 to 0.6 episodes per patient-year and a small but significant decrease in A1C in patients with type 1 diabetes (101). Patient education needs to cover a broad range of information and skill training and often include a motivational element (6).
Short-Term Scrupulous Avoidance of Hypoglycemia
In patients with impaired awareness of hypoglycemia structured patient education should be combined with 2- to 3-weeks of scrupulous avoidance of hypoglycemia – which may require acceptance of somewhat higher glycemic goals in the short-term – since that can be expected to restore awareness of hypoglycemia in most affected patients (54–57).
In summary, people with diabetes treated with a sulfonylurea, a glinide, or insulin should be educated about hypoglycemia, should treat SMPG (or CGM) glucose levels <70 mg/dL (<3.9 mmol/L) to avoid progression to clinical iatrogenic hypoglycemia, and should regularly be queried about hypoglycemia, including the SMPG (or CGM) level at which symptoms develop (6).
TREATMENT OF HYPOGLYCEMIA IN DIABETES
Most episodes of asymptomatic hypoglycemia, detected by routine SMBG or CGM, or of mild- moderate symptomatic hypoglycemia are effectively self-treated by ingestion of glucose tablets or carbohydrate containing juice, soft drinks, candy, other snacks, or a meal (1,104). A reasonable dose is 20 g of carbohydrate (104). The dose can be repeated in 15 to 20 minutes, if necessary. Since the glycemic response to oral glucose is transient – roughly two hours in the setting of ongoing hyperinsulinemia (104) – the ingestion of a more substantial snack or meal shortly after the plasma glucose level is raised is generally advisable.
When a hypoglycemic patient is unwilling (because of neuroglycopenia) or unable to take carbohydrate orally, parenteral therapy is required. That is often glucagon injected subcutaneously or intramuscularly by an associate of the patient who has been trained to recognize and treat severe hypoglycemia. The usual glucagon dose is 1.0 mg; that can be life-saving although it causes substantial, albeit transient, hyperglycemia (104) and can cause nausea, and even vomiting. Smaller doses (e.g., 150 mcg), repeated, if necessary, have been found to be effective without side effects in adolescents (105). Recent advances include 1) approval of nasal glucagon and of a device to deliver glucagon intranasally (106), that would obviate the need for parenteral injection and 2) a glucagon that is stable in solution (107), that would obviate the need to reconstitute the drug prior to administration. Because it also stimulates insulin secretion, glucagon might be less effective in patients with early T2DM. In a medical setting intravenous glucose, 25 g initially, is the standard parenteral therapy (1). The glycemic response to intravenous glucose is, of course, transient. A subsequent glucose infusion is generally needed, and food should be provided as soon as the patient is able to ingest it safely.
The duration of a hypoglycemic episode is a function of its cause. While that caused by a short-acting insulin secretagogue or a rapid-acting insulin can be measured in hours, that caused by a long-acting insulin secretagogue or insulin can last for days requiring hospitalization for prolonged therapy. The duration of secretagogue-induced hypoglycemia can be shortened by administration of octreotide (108,109).
In the UK, the Joint British Diabetes Societies for Inpatient Care have produced guidance on the management of hypoglycemia for hospital inpatients, although these can be used in the community setting as necessary (110).
ACKNOWLEDGMENTS AND DISCLOSURES
Hugh A. Davis has no disclosures to report.
Elias K. Spanakis has received research support (CGM supplies) from DEXCOM (San Diego, CA) for the conduction of inpatient CGM clinical studies.
Maka Siamashvili has no disclosures to report.
Stephen N. Davis- This work has received support from the NIH, NHLBI, NIDDK, JDRF and VA.
REFERENCES
- 1.
- Cryer PE. The barrier of hypoglycemia in diabetes. Vol. 57, Diabetes. 2008. [PMC free article: PMC2584119] [PubMed: 19033403]
- 2.
- Cryer PE. The Prevention and Correction of Hypoglycemia. In: Comprehensive Physiology. 2001.
- 3.
- Cryer PE. Mechanisms of Hypoglycemia-Associated Autonomic Failure in Diabetes. New England Journal of Medicine. 2013;369(4). [PubMed: 23883381]
- 4.
- Cryer PE. Glycemic goals in diabetes: Trade-off between glycemic control and iatrogenic hypoglycemia. Vol. 63, Diabetes. 2014. [PubMed: 24962915]
- 5.
- Cryer PE. Hypoglycemia-associated autonomic failure in diabetes: Maladaptive, adaptive, or both? Vol. 64, Diabetes. 2015. [PMC free article: PMC4876750] [PubMed: 26106190]
- 6.
- Cryer PE. Minimizing hypoglycemia in diabetes. Diabetes Care. 2015;38(8). [PubMed: 26207052]
- 7.
- Shamoon H, others. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Engl J Med. 1993;329. [PubMed: 8366922]
- 8.
- Turner R. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352(9131). [PubMed: 9742976]
- 9.
- Turner R. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet. 1998;352(9131). [PubMed: 9742977]
- 10.
- Intensive Diabetes Treatment and Cardiovascular Disease in Patients with Type 1 Diabetes. New England Journal of Medicine. 2005;353(25). [PMC free article: PMC2637991] [PubMed: 16371630]
- 11.
- Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HAW. 10-Year Follow-up of Intensive Glucose Control in Type 2 Diabetes. New England Journal of Medicine. 2008;359(15). [PubMed: 18784090]
- 12.
- Cryer PE. Hypoglycemia, functional brain failure, and brain death. Vol. 117, Journal of Clinical Investigation. 2007. [PMC free article: PMC1838950] [PubMed: 17404614]
- 13.
- Stahn A, Pistrosch F, Ganz X, Teige M, Koehler C, Bornstein S, et al. Relationship between hypoglycemic episodes and ventricular arrhythmias in patients with type 2 diabetes and cardiovascular diseases: Silent hypoglycemias and silent arrhythmias. Diabetes Care. 2014;37(2). [PubMed: 24041680]
- 14.
- Chow E, Bernjak A, Williams S, Fawdry RA, Hibbert S, Freeman J, et al. Risk of cardiac arrhythmias during hypoglycemia in patients with type 2 diabetes and cardiovascular risk. Diabetes. 2014;63(5). [PubMed: 24757202]
- 15.
- Frier BM, Schernthaner G, Heller SR. Hypoglycemia and cardiovascular risks. Vol. 34, Diabetes Care. 2011. [PMC free article: PMC3632150] [PubMed: 21525444]
- 16.
- Jialal I, Dhindsa S. Hypoglycemia and the predisposition to cardiovascular disease: Is the pro-inflammatory-pro-coagulant diathesis a plausible explanation? Vol. 251, Atherosclerosis. 2016. [PubMed: 27318869]
- 17.
- Lee AK, Warren B, Lee CJ, McEvoy JW, Matsushita K, Huang ES, et al. The association of severe hypoglycemia with incident cardiovascular events and mortality in adults with type 2 diabetes. Diabetes Care. 2018;41(1). [PMC free article: PMC5741158] [PubMed: 29127240]
- 18.
- Mellbin LG. Does hypoglycaemia increase the risk of cardiovascular events? A report from the ORIGIN trial. Eur Heart J. 2013;34(40). [PubMed: 23999452]
- 19.
- Reno CM, Daphna-Iken D, Chen YS, VanderWeele J, Jethi K, Fisher SJ. Severe hypoglycemia-induced lethal cardiac arrhythmias are mediated by sympathoadrenal activation. Diabetes. 2013;62(10). [PMC free article: PMC3781452] [PubMed: 23835337]
- 20.
- Donnelly LA, Morris AD, Frier BM, Ellis JD, Donnan PT, Durran R, et al. Frequency and predictors of hypoglycaemia in Type 1 and insulin-treated Type 2 diabetes: A population-based study. Diabetic Medicine. 2005;22(6). [PubMed: 15910627]
- 21.
- Heller SR, Choudhary P, Davies C, Emery C, Campbell MJ, Freeman J, et al. Risk of hypoglycaemia in types 1 and 2 diabetes: Effects of treatment modalities and their duration. Diabetologia. 2007;50(6). [PubMed: 17415551]
- 22.
- Holstein A, Egberts EH. Risk of Hypoglycaemia with Oral Antidiabetic Agents in Patients with Type 2 Diabetes. Vol. 111, Experimental and Clinical Endocrinology and Diabetes. 2003. [PubMed: 14614647]
- 23.
- 6. Glycemic Targets: Standards of Medical Care in Diabetes—2022. Diabetes Care. 2022;45. [PubMed: 34964868]
- 24.
- Heller SR. Glucose concentrations of less than 3.0 mmol/L (54 mg/dL) should be reported in clinical trials: A joint position statement of the American diabetes association and the European association for the study of diabetes. Diabetes Care. 2017;40(1). [PubMed: 27872155]
- 25.
- Seaquist ER, Anderson J, Childs B, Cryer P, Dagogo-Jack S, Fish L, et al. Hypoglycemia and diabetes: A report of a workgroup of the american diabetes association and the endocrine society. Journal of Clinical Endocrinology and Metabolism. 2013;98(5). [PubMed: 23589524]
- 26.
- Effects of Intensive Glucose Lowering in Type 2 Diabetes. New England Journal of Medicine. 2008;358(24). [PMC free article: PMC4551392] [PubMed: 18539917]
- 27.
- Intensive versus Conventional Glucose Control in Critically Ill Patients. New England Journal of Medicine. 2009;360(13). [PubMed: 19318384]
- 28.
- Giorgino F, Leonardini A, Laviola L. Cardiovascular disease and glycemic control in type 2 diabetes: Now that the dust is settling from large clinical trials. Ann N Y Acad Sci. 2013;1281(1). [PMC free article: PMC3715107] [PubMed: 23387439]
- 29.
- Zoungas S, Patel A, Chalmers J, de Galan BE, Li Q, Billot L, et al. Severe Hypoglycemia and Risks of Vascular Events and Death. New England Journal of Medicine. 2010;363(15). [PubMed: 20925543]
- 30.
- Duckworth W, Abraira C, Moritz T, Reda D, Emanuele N, Reaven PD, et al. Glucose Control and Vascular Complications in Veterans with Type 2 Diabetes. New England Journal of Medicine. 2009;360(2). [PubMed: 19092145]
- 31.
- Davis IC, Ahmadizadeh I, Randell J, Younk L, Davis SN. Understanding the impact of hypoglycemia on the cardiovascular system. Vol. 12, Expert Review of Endocrinology and Metabolism. 2017. [PMC free article: PMC5669378] [PubMed: 29109754]
- 32.
- Robinson RTCE, Harris ND, Ireland RH, Lee S, Newman C, Heller SR. Mechanisms of abnormal cardiac repolarization during insulin-induced hypoglycemia. Diabetes. 2003;52(6). [PubMed: 12765959]
- 33.
- Joy NG, Hedrington MS, Briscoe VJ, Tate DB, Ertl AC, Davis SN. Effects of acute hypoglycemia on inflammatory and pro-atherothrombotic biomarkers in individuals with type 1 diabetes and healthy individuals. Diabetes Care. 2010;33(7). [PMC free article: PMC2890354] [PubMed: 20587723]
- 34.
- Joy NG, Tate DB, Younk LM, Davis SN. Effects of acute and antecedent hypoglycemia on endothelial function and markers of atherothrombotic balance in healthy humans. Diabetes. 2015;64(7). [PMC free article: PMC4477350] [PubMed: 25695946]
- 35.
- Punthakee Z, Miller ME, Launer LJ, Williamson JD, Lazar RM, Cukierman-Yaffee T, et al. Poor cognitive function and risk of severe hypoglycemia in type 2 diabetes: Post hoc epidemiologic analysis of the ACCORD trial. Diabetes Care. 2012;35(4). [PMC free article: PMC3308284] [PubMed: 22374637]
- 36.
- Przezak A, Bielka W, Molęda P. Fear of hypoglycemia—An underestimated problem. Vol. 12, Brain and Behavior. 2022. [PMC free article: PMC9304823] [PubMed: 35620854]
- 37.
- Briscoe VJ, Davis SN. Hypoglycemia in type 1 and type 2 diabetes: Physiology, pathophysiology, and management. Vol. 24, Clinical Diabetes. 2006.
- 38.
- Towler DA, Havlin CE, Craft S, Cryer P. Mechanism of awareness of hypoglycemia: Perception of neurogenic (predominantly cholinergic) rather than neuroglycopenic symptoms. Diabetes. 1993;42(12). [PubMed: 8243825]
- 39.
- DeRosa MA, Cryer PE. Hypoglycemia and the sympathoadrenal system: Neurogenic symptoms are largely the result of sympathetic neural, rather than adrenomedullary, activation. Am J Physiol Endocrinol Metab. 2004;287(1 50-1). [PubMed: 14970007]
- 40.
- Dagogo-Jack SE, Craft S, Cryer PE. Hypoglycemia-associated autonomic failure in insulin-dependent diabetes mellitus: Recent antecedent hypoglycemia reduces autonomic responses to, symptoms of, and defense against subsequent hypoglycemia. Journal of Clinical Investigation. 1993;91(3). [PMC free article: PMC288033] [PubMed: 8450063]
- 41.
- Segel SA, Paramore DS, Cryer PE. Hypoglycemia-associated autonomic failure in advanced type 2 diabetes. Diabetes. 2002;51(3). [PubMed: 11872673]
- 42.
- Gerich JE, Langlois M, Noacco C, Karam JH, Forsham PH. Lack of glucagon response to hypoglycemia in diabetes: Evidence for an intrinsic pancreatic alpha cell defect. Science (1979). 1973;182(4108). [PubMed: 4581053]
- 43.
- Raju B, Cryer PE. Loss of the decrement in intraislet insulin plausibly explains loss of the glucagon response to hypoglycemia in insulin-deficient diabetes: Documentation of the intraislet insulin hypothesis in humans. Diabetes. 2005;54(3). [PubMed: 15734853]
- 44.
- Cooperberg BA, Cryer PE. β-cell-mediated signaling predominates over direct α-cell signaling in the regulation of glucagon secretion in humans. Diabetes Care. 2009;32(12). [PMC free article: PMC2782990] [PubMed: 19729529]
- 45.
- Cryer PE. Mechanisms of sympathoadrenal failure and hypoglycemia in diabetes. Vol. 116, Journal of Clinical Investigation. 2006. [PMC free article: PMC1464914] [PubMed: 16741570]
- 46.
- Heller SR, Cryer PE. Reduced neuroendocrine and symptomatic responses to subsequent hypoglycemia after 1 episode of hypoglycemia in nondiabetic humans. Diabetes. 1991;40(2). [PubMed: 1991573]
- 47.
- Ertl AC, Davis SN. Evidence for a vicious cycle of exercise and hypoglycemia in type 1 diabetes mellitus. Vol. 20, Diabetes/Metabolism Research and Reviews. 2004. [PubMed: 15037987]
- 48.
- Jones TW, Porter P, Sherwin RS, Davis EA, O’Leary P, Frazer F, et al. Decreased Epinephrine Responses to Hypoglycemia during Sleep. New England Journal of Medicine. 1998;338(23). [PubMed: 9614256]
- 49.
- Banarer S, Cryer PE. Sleep-related hypoglycemia-associated autonomic failure in type 1 diabetes: Reduced awakening from sleep during hypoglycemia. Diabetes. 2003;52(5). [PubMed: 12716752]
- 50.
- Schultes B, Jauch-Chara K, Gais S, Hallschmid M, Reiprich E, Kern W, et al. Defective awakening response to nocturnal hypoglycemia in patients with type 1 diabetes mellitus. PLoS Med. 2007;4(2). [PMC free article: PMC1808097] [PubMed: 17326710]
- 51.
- White NH, Skor DA, Cryer PE, Levandoski LA, Bier DM, Santiago J V. Identification of Type I Diabetic Patients at Increased Risk for Hypoglycemia during Intensive Therapy. New England Journal of Medicine. 1983;308(9). [PubMed: 6337335]
- 52.
- Bolli GB, de Feo P, de Cosmo S, Perriello G, Ventura MM, Benedetti MM, et al. A reliable and reproducible test for adequate glucose counterregulation in type I diabetes mellitus. Diabetes. 1984;33(8). [PubMed: 6378698]
- 53.
- Geddes J, Schopman JE, Zammitt NN, Frier BM. Prevalence of impaired awareness of hypoglycaemia in adults with type 1 diabetes. Diabetic Medicine. 2008;25(4). [PubMed: 18387080]
- 54.
- Fanelli CG, Epifano L, Rambotti AM, Pampanelli S, Di Vincenzo A, Modarelli F, et al. Meticulous prevention of hypoglycemia normalizes the glycemic thresholds and magnitude of most of neuroendocrine responses to, symptoms of, and cognitive function during hypoglycemia in intensively treated patients with short-term IDDM. Diabetes. 1993;42(11). [PubMed: 8405713]
- 55.
- Fanelli C, Pampanelli S, Epifano L, Rambotti AM, Di Vincenzo A, Modarelli F, et al. Long-term recovery from unawareness, deficient counterregulation and lack of cognitive dysfunction during hypoglycaemia, following institution of rational, intensive insulin therapy in IDDM. Diabetologia. 1994;37(12). [PubMed: 7895957]
- 56.
- Cranston I, Lomas J, Amiel SA, Maran A, Macdonald I. Restoration of hypoglycaemia awareness in patients with long-duration insulin-dependent diabetes. The Lancet. 1994;344(8918). [PubMed: 7914259]
- 57.
- Dagogo-Jack S, Rattarasarn C, Cryer PE. Reversal of hypoglycemia unawareness, but not defective glucose counterregulation, in IDDM. Diabetes. 1994;43(12). [PubMed: 7958494]
- 58.
- Epidemiology of severe hypoglycemia in the diabetes control and complications trial. Am J Med. 1991;90(1). [PubMed: 2012085]
- 59.
- Gonder-frederick LA, Fisher CD, Ritterband LM, Cox DJ, Hou L, Dasgupta AA, et al. Predictors of fear of hypoglycemia in adolescents with type 1 diabetes and their parents. Pediatr Diabetes. 2006;7(4). [PubMed: 16911009]
- 60.
- Nordfeldt S, Ludvigsson J. Fear and other disturbances of severe hypoglycaemia in children and adolescents with type 1 diabetes mellitus. Journal of Pediatric Endocrinology and Metabolism. 2005;18(1). [PubMed: 15679073]
- 61.
- Cox DJ, Gonder-Frederick L, Ritterband L, Clarke W, Kovatchev BP. Prediction of severe hypoglycemia. Diabetes Care. 2007;30(6). [PubMed: 17363757]
- 62.
- Rossetti P, Porcellati F, Bolli GB, Fanelli CG. Prevention of hypoglycemia while achieving good glycemic control in type 1 diabetes: the role of insulin analogs. Vol. 31 Suppl 2, Diabetes care. 2008. [PubMed: 18227470]
- 63.
- Siebenhofer A, Plank J, Berghold A, Jeitler K, Horvath K, Narath M, et al. Short acting insulin analogues versus regular human insulin in patients with diabetes mellitus. Cochrane Database of Systematic Reviews. 2006. [PubMed: 16625575]
- 64.
- Horvath K, Jeitler K, Berghold A, Ebrahim SH, Gratzer TW, Plank J, et al. Long-acting insulin analogues versus NPH insulin (human isophane insulin) for type 2 diabetes mellitus. Cochrane Database of Systematic Reviews. 2007. [PubMed: 17443605]
- 65.
- Pedersen-Bjergaard U, Kristensen PL, Beck-Nielsen H, Nørgaard K, Perrild H, Christiansen JS, et al. Effect of insulin analogues on risk of severe hypoglycaemia in patients with type 1 diabetes prone to recurrent severe hypoglycaemia (HypoAna trial): A prospective, randomised, open-label, blinded-endpoint crossover trial. Lancet Diabetes Endocrinol. 2014;2(7). [PubMed: 24794703]
- 66.
- Garber AJ, King AB, Del Prato S, Sreenan S, Balci MK, Muñoz-Torres M, et al. Insulin degludec, an ultra-longacting basal insulin, versus insulin glargine in basal-bolus treatment with mealtime insulin aspart in type 2 diabetes (BEGIN Basal-Bolus Type 2): A phase 3, randomised, open-label, treat-to-target non-inferiority trial. The Lancet. 2012;379(9825). [PubMed: 22521072]
- 67.
- Eng C, Kramer CK, Zinman B, Retnakaran R. Glucagon-like peptide-1 receptor agonist and basal insulin combination treatment for the management of type 2 diabetes: A systematic review and meta-analysis. The Lancet. 2014;384(9961). [PubMed: 25220191]
- 68.
- Fatourechi MM, Kudva YC, Murad MH, Elamin MB, Tabini CC, Montori VM. Hypoglycemia with intensive insulin therapy: A systematic review and meta-analyses of randomized trials of continuous subcutaneous insulin infusion versus multiple daily injections. Vol. 94, Journal of Clinical Endocrinology and Metabolism. 2009. [PubMed: 19088167]
- 69.
- Yeh HC, Brown TT, Maruthur N, Ranasinghe P, Berger Z, Suh YD, et al. Comparative effectiveness and safety of methods of insulin delivery and glucose monitoring for diabetes mellitus: A systematic review and meta-analysis. Vol. 157, Annals of Internal Medicine. 2012. [PubMed: 22777524]
- 70.
- Pickup JC, Reznik Y, Sutton AJ. Glycemic control during continuous subcutaneous insulin infusion versus multiple daily insulin injections in type 2 diabetes: Individual patient Data meta-analysis and meta-regression of randomized controlled trials. Diabetes Care. 2017;40(5). [PubMed: 28428322]
- 71.
- Benkhadra K, Alahdab F, Tamhane SU, McCoy RG, Prokop LJ, Murad MH. Continuous subcutaneous insulin infusion versus multiple daily injections in individuals with type 1 diabetes: a systematic review and meta-analysis. Endocrine. 2017;55(1). [PubMed: 27477293]
- 72.
- Beck RW, Riddlesworth T, Ruedy K, Ahmann A, Bergenstal R, Haller S, et al. Effect of continuous glucose monitoring on glycemic control in adults with type 1 diabetes using insulin injections the diamond randomized clinical trial. In: JAMA - Journal of the American Medical Association. 2017. [PubMed: 28118453]
- 73.
- Beck RW, Riddlesworth TD, Ruedy K, Ahmann A, Haller S, Kruger D, et al. Continuous glucose monitoring versus usual care in patients with type 2 diabetes receiving multiple daily insulin injections. Ann Intern Med. 2017;167(6). [PubMed: 28828487]
- 74.
- US Food and Drug Administration. Press Announcements - FDA expands indication for continuous glucose monitoring system, first to replace fingerstick testing for diabetes treatment decisions. FDA News Release. 2016.
- 75.
- News Release F. FDA Approves First Continuous Glucose Monitoring System for Adults Not Requiring Blood Sample Calibration. Vol. 9, Molecular and Cellular Pharmacology. 2017.
- 76.
- Rickels MR, Peleckis AJ, Dalton-Bakes C, Naji JR, Ran NA, Nguyen HL, et al. Continuous glucose monitoring for hypoglycemia avoidance and glucose counterregulation in long-standing type 1 diabetes. Journal of Clinical Endocrinology and Metabolism. 2018;103(1). [PMC free article: PMC6283439] [PubMed: 29190340]
- 77.
- Cooper MN, O’Connell SM, Davis EA, Jones TW. A population-based study of risk factors for severe hypoglycaemia in a contemporary cohort of childhood-onset type 1 diabetes. Diabetologia. 2013;56(10). [PubMed: 23832082]
- 78.
- Johnson SR, Cooper MN, Jones TW, Davis EA. Long-term outcome of insulin pump therapy in children with type 1 diabetes assessed in a large population-based case-control study. Diabetologia. 2013;56(11). [PubMed: 23963323]
- 79.
- Bergenstal RM, Klonoff DC, Garg SK, Bode BW, Meredith M, Slover RH, et al. Threshold-Based Insulin-Pump Interruption for Reduction of Hypoglycemia. New England Journal of Medicine. 2013;369(3). [PubMed: 23789889]
- 80.
- Ly TT, Nicholas JA, Retterath A, Lim EM, Davis EA, Jones TW. Effect of sensor-augmented insulin pump therapy and automated insulin suspension vs standard insulin pump therapy on hypoglycemia in patients with type 1 diabetes: A randomized clinical trial. JAMA. 2013;310(12). [PubMed: 24065010]
- 81.
- Maahs DM, Calhoun P, Buckingham BA, Chase HP, Hramiak I, Lum J, et al. A randomized trial of a home system to reduce nocturnal hypoglycemia in type 1 diabetes. Diabetes Care. 2014;37(7). [PMC free article: PMC4067393] [PubMed: 24804697]
- 82.
- Leelarathna L, Dellweg S, Mader JK, Allen JM, Benesch C, Doll W, et al. Day and night home closed-loop insulin delivery in adults with type 1 diabetes: Three-center randomized crossover study. Diabetes Care. 2014;37(7). [PubMed: 24963110]
- 83.
- Russell SJ, El-Khatib FH, Sinha M, Magyar KL, McKeon K, Goergen LG, et al. Outpatient Glycemic Control with a Bionic Pancreas in Type 1 Diabetes. New England Journal of Medicine. 2014;371(4). [PMC free article: PMC4183762] [PubMed: 24931572]
- 84.
- Ang M, Meyer C, Brendel MD, Bretzel RG, Linn T. Magnitude and mechanisms of glucose counterregulation following islet transplantation in patients with type 1 diabetes suffering from severe hypoglycaemic episodes. Diabetologia. 2014;57(3). [PubMed: 24305963]
- 85.
- FDA. FDA. 2020. FDA Approves First-of-its-Kind Automated Insulin Delivery and Monitoring System for Use in Young Pediatric Patients.
- 86.
- Tansey MJ, Tsalikian E, Beck RW, Mauras N, Buckingham BA, Weinzimer SA, et al. The effects of aerobic exercise on glucose and counterregulatory hormone concentrations in children with type 1 diabetes. Diabetes Care. 2006;29(1). [PMC free article: PMC2396943] [PubMed: 16373890]
- 87.
- MacDonald MJ. Postexercise late-onset hypoglycemia in insulin-dependent diabetic patients. Diabetes Care. 1987;10(5). [PubMed: 3677976]
- 88.
- Tsalikian E. Impact of exercise on overnight glycemic control in children with type 1 diabetes mellitus. Journal of Pediatrics. 2005;147(4). [PMC free article: PMC2258153] [PubMed: 16227041]
- 89.
- Gallen IW. Hypoglycemia associated with exercise in people with type 1 diabetes. Vol. 7, Diabetic Hypoglycemia. 2014.
- 90.
- Raju B, Arbelaez AM, Breckenridge SM, Cryer PE. Nocturnal hypoglycemia in type 1 diabetes: An assessment of preventive bedtime treatments. Journal of Clinical Endocrinology and Metabolism. 2006;91(6). [PubMed: 16492699]
- 91.
- Cooperberg BA, Breckenridge SM, Arbelaez AM, Cryer PE. Terbutaline and the prevention of nocturnal hypoglycemia in type 1 diabetes. Diabetes Care. 2008;31(12). [PMC free article: PMC2584177] [PubMed: 18782903]
- 92.
- Taplin CE, Cobry E, Messer L, McFann K, Chase HP, Fiallo-Scharer R. Preventing post-exercise nocturnal hypoglycemia in children with type 1 diabetes. Journal of Pediatrics. 2010;157(5). [PMC free article: PMC2957531] [PubMed: 20650471]
- 93.
- Elsayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, et al. 13. Older Adults: Standards of Care in Diabetes—2023. Diabetes Care. 2023;46. [PMC free article: PMC9810468] [PubMed: 36507638]
- 94.
- Cox DJ, Singh H, Lorber D. Diabetes and driving safety: Science, ethics, legality and practice. In: American Journal of the Medical Sciences. 2013. [PMC free article: PMC3652323] [PubMed: 23531955]
- 95.
- Nielsen LR, Pedersen-Bjergaard U, Thorsteinsson B, Johansen M, Damm P, Mathiesen ER. Hypoglycemia in pregnant women with type 1 diabetes: Predictors and role of metabolic control. Diabetes Care. 2008;31(1). [PubMed: 17909091]
- 96.
- Inzucchi SE, Bergenstal RM, Buse JB, Diamant M, Ferrannini E, Nauck M, et al. Management of Hyperglycemia in Type 2 Diabetes, 2015: A Patient-Centered Approach: Update to a position statement of the american diabetes association and the european association for the study of diabetes. Diabetes Care. 2015;38(1). [PubMed: 25538310]
- 97.
- Children and adolescents: Standards of medical care in diabetes- 2020. Diabetes Care. 2020;43. [PubMed: 31862756]
- 98.
- Sämann A, Mühlhauser I, Bender R, Kloos C, Müller UA. Glycaemic control and severe hypoglycaemia following training in flexible, intensive insulin therapy to enable dietary freedom in people with type 1 diabetes: A prospective implementation study. Diabetologia. 2005;48(10). [PubMed: 16132954]
- 99.
- Little SA, Leelarathna L, Walkinshaw E, Tan HK, Chapple O, Lubina-Solomon A, et al. Recovery of hypoglycemia awareness in long-standing type 1 diabetes: A multicenter 2 × 2 factorial randomized controlled trial comparing insulin pump with multiple daily injections and continuous with conventional glucose self-monitoring (HypoCOMPaSS). Diabetes Care. 2014;37(8). [PubMed: 24854041]
- 100.
- Leelarathna L, Little SA, Walkinshaw E, Tan HK, Lubina-Solomon A, Kumareswaran K, et al. Restoration of self-awareness of hypoglycemia in adultswith long-standing type 1 diabetes: Hyperinsulinemic-hypoglycemic clamp substudy results from the HypoCOMPaSS trial. Diabetes Care. 2013;36(12). [PMC free article: PMC3836150] [PubMed: 24130355]
- 101.
- Hopkins D, Lawrence IAN, Mansell P, Thompson G, Amiel S, Campbell M, et al. Improved biomedical and psychological outcomes 1 year after structured education in flexible insulin therapy for people with type 1 diabetes the U.K. DAFNE experience. Diabetes Care. 2012;35(8). [PMC free article: PMC3402270] [PubMed: 22619082]
- 102.
- De Zoysa N, Rogers H, Stadler M, Gianfrancesco C, Beveridge S, Britneff E, et al. A psychoeducational program to restore hypoglycemia awareness: The DAFNE-HART pilot study. Diabetes Care. 2014;37(3). [PubMed: 24319119]
- 103.
- Elliott J, Jacques RM, Kruger J, Campbell MJ, Amiel SA, Mansell P, et al. Substantial reductions in the number of diabetic ketoacidosis and severe hypoglycaemia episodes requiring emergency treatment lead to reduced costs after structured education in adults with Type 1 diabetes. Diabetic Medicine. 2014;31(7). [PMC free article: PMC4264891] [PubMed: 24654672]
- 104.
- Wiethop B V., Cryer PE. Alanine and terbutaline in treatment of hypoglycemia in IDDM. Diabetes Care. 1993;16(8). [PubMed: 8375243]
- 105.
- Haymond MW, Schreiner B. Mini-dose glucagon rescue for hypoglycemia in children with type 1 diabetes. Diabetes Care. 2001;24(4). [PubMed: 11315823]
- 106.
- Pontiroli AE. Intranasal glucagon: A promising approach for treatment of severe hypoglycemia. J Diabetes Sci Technol. 2015;9(1). [PMC free article: PMC4495544] [PubMed: 25385946]
- 107.
- Chabenne J, Chabenne MDM, Zhao Y, Levy J, Smiley D, Gelfanov V, et al. A glucagon analog chemically stabilized for immediate treatment of life-threatening hypoglycemia. Mol Metab. 2014;3(3). [PMC free article: PMC3986664] [PubMed: 24749059]
- 108.
- Boyle PJ, Justice K, Krentz AJ, Nagy RJ, Schade DS. Octreotide reverses hyperinsulinemia and prevents hypoglycemia induced by sulfonylurea overdoses. Journal of Clinical Endocrinology and Metabolism. 1993;76(3). [PubMed: 8445035]
- 109.
- McLaughlin SA, Crandall CS, McKinney PE. Octreotide: An antidote for sulfonylurea-induced hypoglycemia. Ann Emerg Med. 2000;36(2). [PubMed: 10918104]
- 110.
- Graveling A, Walden E, Flanagan D. The Hospital Management of Hypoglycaemia in Adults with Diabetes Mellitus. Joint British Diabetes Societies for Inpatient Care. 2022.
- ABSTRACT
- THE CLINICAL PROBLEM OF HYPOGLYCEMIA IN DIABETES
- DEFINITION AND CLASSIFICATION OF HYPOGLYCEMIA
- COMPLICATIONS OF HYPOGLYCEMIA
- GLUCOSE COUNTERREGULATORY PHYSIOLOGY AND ITS PATHOPHYSIOLOGY IN DIABETES
- RISK FACTORS FOR HYPOGLYCEMIA IN DIABETES
- PREVENTION OF HYPOGLYCEMIA IN DIABETES
- TREATMENT OF HYPOGLYCEMIA IN DIABETES
- ACKNOWLEDGMENTS AND DISCLOSURES
- REFERENCES
- Review Hypoglycemia risk reduction in type 1 diabetes.[Exp Clin Endocrinol Diabetes. ...]Review Hypoglycemia risk reduction in type 1 diabetes.Cryer PE. Exp Clin Endocrinol Diabetes. 2001; 109 Suppl 2:S412-23.
- Review The science of hypoglycemia in patients with diabetes.[Curr Diabetes Rev. 2013]Review The science of hypoglycemia in patients with diabetes.Oyer DS. Curr Diabetes Rev. 2013 May; 9(3):195-208.
- Review Minimizing Hypoglycemia in Diabetes.[Diabetes Care. 2015]Review Minimizing Hypoglycemia in Diabetes.International Hypoglycaemia Study Group. Diabetes Care. 2015 Aug; 38(8):1583-91.
- Review Hypoglycemia in diabetes.[Diabetes Care. 2003]Review Hypoglycemia in diabetes.Cryer PE, Davis SN, Shamoon H. Diabetes Care. 2003 Jun; 26(6):1902-12.
- Review Hypoglycemia in diabetes: pathophysiological mechanisms and diurnal variation.[Prog Brain Res. 2006]Review Hypoglycemia in diabetes: pathophysiological mechanisms and diurnal variation.Cryer PE. Prog Brain Res. 2006; 153:361-5.
- Hypoglycemia During Therapy of Diabetes - EndotextHypoglycemia During Therapy of Diabetes - Endotext
- BARHL2 [Pongo abelii]BARHL2 [Pongo abelii]Gene ID:100458718Gene
- STK_RS06050 [Sulfurisphaera tokodaii str. 7]STK_RS06050 [Sulfurisphaera tokodaii str. 7]Gene ID:1459078Gene
- IGFL1 IGF like family member 1 [Homo sapiens]IGFL1 IGF like family member 1 [Homo sapiens]Gene ID:374918Gene
- Csnk1g1 casein kinase 1, gamma 1 [Mus musculus]Csnk1g1 casein kinase 1, gamma 1 [Mus musculus]Gene ID:214897Gene
Your browsing activity is empty.
Activity recording is turned off.
See more...