NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
Dean L. Blood Groups and Red Cell Antigens [Internet]. Bethesda (MD): National Center for Biotechnology Information (US); 2005.
The average human adult has more than 5 liters (6 quarts) of blood in his or her body. Blood carries oxygen and nutrients to living cells and takes away their waste products. It also delivers immune cells to fight infections and contains platelets that can form a plug in a damaged blood vessel to prevent blood loss.
Through the circulatory system, blood adapts to the body's needs. When you are exercising, your heart pumps harder and faster to provide more blood and hence oxygen to your muscles. During an infection, the blood delivers more immune cells to the site of infection, where they accumulate to ward off harmful invaders.
All of these functions make blood a precious fluid. Each year in the USA, 30 million units of blood components are transfused to patients who need them. Blood is deemed so precious that is also called "red gold" because the cells and proteins it contains can be sold for more than the cost of the same weight in gold.
This chapter introduces the components of blood.
Blood contains cells, proteins, and sugars
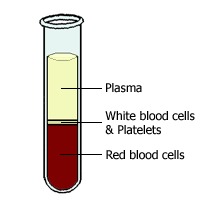
The straw-colored fluid that forms the top layer is called plasma and forms about 60% of blood. The middle white layer is composed of white blood cells (WBCs) and platelets, and the bottom red layer is the red blood cells (RBCs). These bottom two layers of cells form about 40% of the blood.
Plasma is mainly water, but it also contains many important substances such as proteins (albumin, clotting factors, antibodies, enzymes, and hormones), sugars (glucose), and fat particles.
All of the cells found in the blood come from bone marrow. They begin their life as stem cells, and they mature into three main types of cells— RBCs, WBCs, and platelets. In turn, there are three types of WBC—lymphocytes, monocytes, and granulocytes—and three main types of granulocytes (neutrophils, eosinophils, and basophils). See them in action in "Meet the blood cells".
See a figure of all the cellular elements of blood in Janeway & Traver's Immunobiology
A sample of blood can be further separated into its individual components by spinning the sample in a centrifuge. The force of the spinning causes denser elements to sink, and further processing enables the isolation of a particular protein or the isolation of a particular type of blood cell. With the use of this method, antibodies and clotting factors can be harvested from the plasma to treat immune deficiencies and bleeding disorders, respectively. Likewise, RBCs can be harvested for blood transfusion.
Red blood cells transport oxygen

In humans, as in all mammals, the mature RBC lacks a nucleus. This allows the cell more room to store hemoglobin, the oxygen-binding protein, enabling the RBC to transport more oxygen. RBCs are also biconcave in shape; this shape increases their surface area for the diffusion of oxygen across their surfaces. In non-mammalian vertebrates such as birds and fish, mature RBCs do have a nucleus.
See an electron micrograph of red blood cells in Albert's
Molecular Biology of the Cell
If a patient has a low level of hemoglobin, a condition called anemia, they may appear pale because hemoglobin gives RBCs, and hence blood, their red color. They may also tire easily and feel short of breath because of the essential role of hemoglobin in transporting oxygen from the lungs to wherever it is needed around the body.
White blood cells are part of the immune response
WBCs come in many different shapes and sizes. Some cells have nuclei with multiple lobes, whereas others contain one large, round nucleus. Some contain packets of granules in their cytoplasm and so are known as granulocytes.
See an electron micrograph of white blood cells in Albert's
Molecular Biology of the Cell
Despite their differences in appearance, all of the various types of WBCs have a role in the immune response. They circulate in the blood until they receive a signal that a part of the body is damaged. Signals include interleukin 1 (IL-1), a molecule secreted by macrophages that contributes to the fever of infections, and histamine, which is released by circulating basophils and tissue mast cells, and contributes to allergic reactions. In response to these signals, the WBCs leave the blood vessel by squeezing through holes in the blood vessel wall. They migrate to the source of the signal and help begin the healing process.
Individuals who have low levels of WBCs may have more and worse infections. Depending upon which WBCs are missing, the patient is at risk for different types of infection. For example, macrophages are especially good at swallowing bacteria, and a deficiency in macrophages leads to recurrent bacterial infections. In contrast, T cells are particularly skilled in fighting viral infections, and a loss of their function results in an increased susceptibility to viral infections.
Neutrophils digest bacteria

See a neutrophil phagocytose a bacterium in Albert's
Molecular Biology of the Cell
Monocytes become macrophages

In the liver, tissue macrophages are called Kupffer cells, and they specialize in removing harmful agents from blood that has left the gut. Alveolar macrophages are in the lungs and remove harmful agents that may have been inhaled. Macrophages in the spleen remove old or damaged red blood cells and platelets from the circulation.
See a macrophage phagocytose a red blood cell in Albert's
Molecular Biology of the Cell
Macrophages are also "antigen-presenting cells", presenting the foreign proteins (antigens) to other immune cells, triggering an immune response.
Lymphocytes consist of B cells and T cells

See an electron micrograph of a B cell and T cell in Albert's
Molecular Biology of the Cell
Once activated, the B cells and T cells trigger different types of immune response. The activated B cells, also known as plasma cells, produce highly specific antibodies that bind to the agent that triggered the immune response. T cells, called helper T cells, secrete chemicals that recruit other immune cells and help coordinate their attack. Another group, called cytotoxic T cells, attacks virally infected cells.
Platelets help blood to clot

A diagram of a platelet in Albert's
Molecular Biology of the Cell
As with all the cells in the blood, platelets originate from stem cells in the bone marrow. The stem cells develop into platelet precursors (called megakaryocytes) that "shed" platelets into the bloodstream. There, platelets circulate for about 9 days. If they encounter damaged blood vessel walls during this time, they stick to the damaged area and are activated to form a blood clot. This plugs the hole. Otherwise, at the end of their life span they are removed from the circulation by the spleen. In a diverse number of diseases where the spleen is overactive, e.g. rheumatoid arthritis and leukemia, the spleen removes too many platelets, leading to increased bleeding.
Your complete blood count
A complete blood count (CBC) is a simple blood test that is commonly ordered as part of a routine medical assessment. As the name suggests, it is a count of the different types of cells found in the blood. The test can diagnose and monitor many different diseases, such as anemia, infection, inflammatory diseases, and malignancy. Table 1 gives an example of CBC values, but note that the reference ranges and the units used may differ, depending upon the laboratory that carried out the test.
Red blood cell count detects anemia
A CBC measures the following features of RBCs:
- the total amount of hemoglobin (Hb) in the blood
- the number of RBCs (RBCs)
- the average size of a RBC (MCV)
- the amount of space RBCs take up in the blood (hematocrit)
The CBC also includes information about RBCs that is calculated from the other measurements, e.g., the amount (MCH) and concentration (MCHC) of hemoglobin in RBCs.
The number of RBCs and the amount of hemoglobin in the blood are lower in women than in men. This is because of the menstrual loss of blood each month. Below a certain level of hemoglobin, a patient is said to be anemic, suggesting a clinically significant drop in oxygen carrying capacity. Anemia is not a diagnosis but a symptom of an underlying disease that has to be investigated.
A clue to the cause of anemia is the average size of RBC (mean corpuscular volume, MCV). Causes of a high MCV include a deficiency of B12 or folate vitamins in the diet. B12 is found in red meat therefore, a deficiency of B12 is especially common in vegetarians and vegans. Conversely, folate is plentiful in fresh leafy green vegetables, therefore, a deficiency of folate is common in the elderly, who may have a poor diet.
Low MCV anemia is common and may be a result of hereditary blood disorders, such as thalassemia, but is most often caused by a deficiency of iron. For example, women of reproductive age may lose too much iron through heavy menstrual bleeding and are prone to this form of anemia, known as iron-deficiency anemia.
Hematocrit is the percentage of RBCs in relation to the total volume of blood
The hematocrit measures the fraction of the blood that is made up of RBCs. It reflects the combination of the total number of RBCs, and the volume that they occupy.
One of the changes seen in pregnancy is a drop in hematocrit. This occurs because although the production of RBCs does not change greatly, the plasma volume increases, i.e., the RBCs are "diluted". Alternatively, a low hematocrit can reflect a drop in RBC production by the bone marrow. This may be attributable to bone marrow disease (damage by toxins or cancer) or due to a decrease in erythropoietin, a hormone secreted by the kidney that stimulates RBC production. Decreased RBCs may also be the result of a reduced life span of the RBCs (e.g., chronic bleeding).
A high hematocrit value may truly reflect an increase in the fraction of RBCs (e.g., increased erythropoietin attributable to a tumor of RBCs called polycythemia rubra vera), or it may reflect a drop in the plasma component of the blood (e.g., fluid loss in burn victims).
The number of WBCs increases in infection and tumors
The WBC count is a count of the number of WBCs found in one cubic millimeter of blood.
An increased number of WBCs is most commonly caused by infections, such as a urinary tract infection or pneumonia. It may also be caused by WBC tumors, such as leukemia.
A decreased number of WBCs is caused by the bone marrow failing to produce WBCs or by an increased removal of WBCs from the circulation by a diseased liver or an overactive spleen. Bone marrow failure may be caused by toxins or by the normal bone marrow cells being replaced by tumor cells.
The WBC differential part of the CBC breaks down the WBCs into five different types: neutrophils, lymphocytes, monocytes, eosinophils, and basophils. Finding out the count of each type of WBC gives more information about the underlying problem. For example, in the early stages of an infection, most of the increase in WBCs is attributable to the increase in neutrophils. As the infection continues, lymphocytes increase. Worm infections can trigger an increase in eosinophils, whereas allergic conditions, such as hay fever, trigger an increase in basophils.
The number of platelets indicates whether bleeding or clotting is likely
Normally, one cubic millimeter of blood contains between 150,000 and 400,000 platelets. If the number drops below this range, uncontrolled bleeding becomes a risk, whereas a rise above the upper limit of this range indicates a risk of uncontrolled blood clotting.
Hemoglobin binds oxygen
Hemoglobin is the oxygen-carrying protein that is found within all RBCs. It picks up oxygen where it is abundant (the lungs) and drops off oxygen where it is needed around the body. Hemoglobin is also the pigment that gives RBCs their red color.
Heme groups and globins
As its name suggests, hemoglobin is composed of "heme" groups (iron-containing rings) and "globins" (proteins). In fact, hemoglobin is composed of four globin proteins—two alpha chains and two beta chains—each with a heme group. The heme group contains one iron atom, and this can bind one molecule of oxygen. Because each molecule of hemoglobin contains four globins, it can carry up to four molecules of oxygen.
See hemoglobin structure in Albert's
Molecular Biology of the Cell
Hemoglobin transports oxygen
In the lungs, a hemoglobin molecule is surrounded by a high concentration of oxygen, therefore, it binds oxygen. In active tissues, the oxygen concentration is lower, so hemoglobin releases its oxygen.
This behavior is much more effective because the hemoglobin––oxygen binding is "co-operative". This means that the binding of one molecule of oxygen makes it easier for the binding of subsequent oxygen molecules. Likewise, the unbinding of oxygen makes it easier for other oxygen molecules to be released. This means that the response of hemoglobin to the oxygen needs of active tissues is much quicker.
Aside from the oxygen saturation of hemoglobin, other factors that influence how readily hemoglobin binds oxygen include plasma pH, plasma bicarbonate levels, and the pressure of oxygen in the air (high altitudes in particular).
The molecule 2,3-disphosphoglycerate (2,3-DPG ) binds to hemoglobin and lowers its affinity for oxygen, thus promoting oxygen release. In individuals who have become acclimatized to living at high altitudes, the level of 2,3-DPG in the blood increases, allowing the delivery of more oxygen to tissues under low oxygen tension.
Fetal hemoglobin
Fetal hemoglobin differs from adult hemoglobin in that it contains two gamma chains instead of two beta chains. Fetal hemoglobin binds oxygen with a much greater affinity than adult hemoglobin; this is an advantage in the womb because it allows fetal blood to extract oxygen from maternal blood, despite its low concentration of oxygen.
Normally, all fetal hemoglobin is replaced by adult hemoglobin by the time of birth.
Breaking down hemoglobin
Old or damaged RBCs are removed from the circulation by macrophages in the spleen and liver, and the hemoglobin they contain is broken down into heme and globin. The globin protein may be recycled, or broken down further to its constituent amino acids, which may be recycled or metabolized. The heme contains precious iron that is conserved and reused in the synthesis of new hemoglobin molecules.
During its metabolism, heme is converted to bilirubin, a yellow pigment that can discolor the skin and sclera of the eye if it accumulates in the blood, a condition known as jaundice. Instead, the plasma protein albumin binds to bilirubin and carries it to the liver, where it is secreted in bile and also contributes to the color of feces.
Jaundice is one of the complications of an incompatible blood transfusion. This occurs when the recipient's immune system attacks the donor RBCs as being foreign. The rate of RBC destruction and subsequent bilirubin production can exceed the capacity of the liver to metabolize the bilirubin produced.
Hemoglobinopathies
Hemoglobinopathies form a group of inherited diseases that are caused by mutations in the globin chains of hemoglobin. Sickle cell anemia is the most common of these and is attributable to a mutation that changes one of the amino acids in the hemoglobin beta chain, producing hemoglobin that is "fragile". When the oxygen concentration is low, RBCs tend to become distorted and "sickle" shaped. These deformed cells can block small blood vessels and damage the organs they are supplying. This can be very painful, and if not treated, a sickle cell crisis can be fatal.
Sickle cell anemia in Genes and Disease
Another inherited anemia that particularly affects individuals of Mediterranean descent is thalassemia. A fault in the production of either alpha or beta globin chains causes a range of symptoms, depending on how many copies of the alpha and beta genes are affected. Some individuals may be carriers of the disease and have no symptoms, whereas if all copies of the genes are lost, the disease is fatal.
Thalassemia in Genes and Disease
The porphyrias are a group of inherited disorders in which the synthesis of heme is disrupted. Depending upon the stage at which the disruption occurs, there are a range of neurological and gastrointestinal side effects. King George III of England ("the madness of King George") was one of the most famous individuals who suffered from porphyria.
Porphyria in Genes and Disease
Resources
Karl Landsteiner, Nobel Laureate from Nobelprize.org
Red Gold: the epic story of blood from Public Broadcasting Service (PBS)
Tables
Table 1Complete blood count
| Blood component | Abbreviation used | Reference range | SI Reference range |
|---|---|---|---|
| White blood cells | WBC | 4500-11,000/mm3 | 4.5-11.0 x 109/L |
| Red blood cells* | RBC | Male: 4.3-5.9
million/mm3 Female: 3.5-5.5 million/mm3 | Male: 4.3-5.9 x
1012/L Female: 3.5-5.5 x 1012/L |
| Hemoglobin* | HGB | Male: 13.5-17.5 g/dL Female: 12.0-16.0 g/dL | Male: 2.09-2.71 mmol/L Female: 1.86-2.48 mmol/L |
| Hematocrit* | HT | Male: 41%-53% Female: 36%-46% | Male: 0.41-0.53 Female: 0.36-0.46 |
| Mean corpuscular volume | MCV | 80-100 µm3 | 80-100 fl |
| Mean corpuscular hemoglobin | MCH | 25.4-34.6 pg/cell | 0.39-0.54 fmol/cell |
| Mean corpuscular hemoglobin concentration | MCHC | 31%-36% Hb/cell | 4.81-5.58 mmol Hb/L |
| Platelets | Platelets | 150,000-400,000/mm3 | 150-400 x 109/L |
*Values differ depending upon altitude.
Boxes
Meet the blood cells
Click on the cells to find out more about them.
To view "Meet the blood cells", you will need to have Flash installed on your computer.