

NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-.

ABSTRACT
Sitosterolemia is a rare autosomal recessive disorder of non-cholesterol sterol metabolism, caused by mutations of the ABCG5 or ABCG8 transporter genes. This results in hyperabsorption and decreased biliary excretion of non-cholesterol sterol, especially sitosterol, from the gastrointestinal tract. Affected individuals have excessive accumulation of plant sterols and 5 alpha-saturated stanols in plasma and tissues, resulting in premature cardiovascular disease. The condition is often clinically confused with familial hypercholesterolemia. This article provided overview of this rare condition, including diagnostic evaluation and treatment. For complete coverage of all related areas of Endocrinology, please visit our on-line FREE web-text, WWW.ENDOTEXT.ORG.
BACKGROUND
Sterols are waxy insoluble substances and are synthesized from acetyl coenzyme A (CoA). Perhaps the most familiar example is cholesterol. In addition to cholesterol, over forty non-cholesterol sterols are also present in the human diet. Non-cholesterol sterols are contained in plants, fungi, and yeast. Instead of converting squalene to cholesterol, non-cholesterol sterols occur when squalene is converted to stigmasterol, sitosterol, campesterol, ergosterol, etc., while shellfish produce fucosterol.
In a typical Western diet, plant sterols, or phytosterols, are often consumed in nuts, seeds, legumes, and vegetable oils. They are present in amounts equal to cholesterol and processed by the intestine in a similar manner (Figure 1). While most individuals absorb, on average, 40-50% of dietary cholesterol, less than 5% of dietary plant sterols are absorbed (1-3).
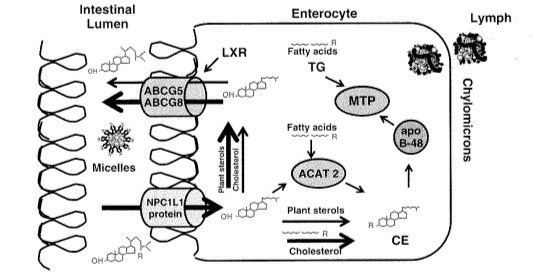
Figure 1.
Enterocyte Trafficking of Cholesterol and Plant Sterols. From Phytoserolemia by Thomas Daysring, MD in Therapeutic Lipidology, Michael H Davis in, MD, Peter P Toth, MD and Kevin C Maki, PhD, Editors. 2007 Humana Press, Incorp. Totowa, New Jersey.
Phytosterols have no role in human metabolism. Therefore, except in inherited disorders of metabolism, there is limited systemic absorption of phytosterols, as their entry into the plasma is highly regulated by the intestine and liver. Concentrations of phystosterols in plasma are normally less than 0.5% that of cholesterol.
Stanols, i.e., saturated sterols, also exist in the diet, primarily from plant sources. Stanols are not normally absorbed from the GI tract. Both stanols and sterols interfere with the absorption of cholesterol. Therefore, both have been used as dietary supplements for over 5 decades to help reduce plasma cholesterol levels.
Phytosterols and free cholesterol are normally absorbed by the Niemann-Pick C1-Like 1 (NPC1L1) protein expressed on enterocytes (Figure 1) (4). Almost all of the absorbed plant phytosterols are excreted back into the intestinal lumen by the ABCG5 or ABCG8 transporters. The normal body is thus able to discriminate between cholesterol and non-cholesterol sterols (5). The function of ABCG5 or ABCG8 transporter genes, found at the STSL locus of human chromosome 2p21, is to limit intestinal absorption and promote biliary excretion (6, 7) (Figure 2).
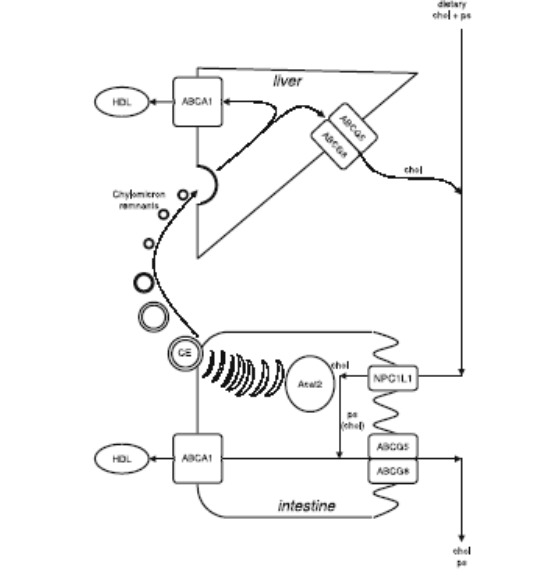
Figure 2.
Normal Intestinal and Hepatic Transport of Cholesterol and Phytosterols. T. Plösch, A. Kosters, A.K. Groen, F. Kuipers. The ABC of Hepatic and Intestinal Cholesterol Transport. Chapter. Atherosclerosis: Diet and Drugs. Volume 170 of the series Handbook of Experimental Pharmacology pp 465-482.
SITOSTEROLEMIA
Sitosterolemia (also known as phytosterolemia) is a rare autosomal recessive disease of non-cholesterol sterol metabolism. It is characterized chemically by the accumulation of plant sterols and 5 alpha-saturated stanols in plasma and tissues. The condition occurs when either ABCG5 or ABCG8 are defective, leading to hyperabsorption of sitosterol from the gastrointestinal tract. The problem is compounded by decreased biliary excretion, resulting in accumulation of dietary phytosterols in different tissues (8, 9).
HISTORY AND ETHNICITY
Sitosterolemia was first reported in 1974 when two sisters with extensive tendon xanthomas were found to have normal plasma cholesterol levels and elevated levels of plant sterols (10). Several hundred cases have since been reported but the condition is thought to be substantially underdiagnosed (11). The disorder has been found in a wide range of diverse populations, including the Old-Order Amish, Chinese, Finnish, Japanese, Norwegian, Indian and Caucasian South Africans, as well as others. The condition is transmitted as an autosomal recessive trait (12, 13)
CLINICAL FEATURES
Signs and Symptoms
Phenotypically, sitosterolemia is very heterogeneous in its presentation. The disorder is characterized by premature coronary artery disease (14-18) although the degree of atherosclerosis present varies significantly (19-24). Presenting signs and symptoms of sitosterolemia, such as lipid deposition in cutaneous and subcutaneous structures (xanthomas), can occur in the first decade of life, but sitosterolemia has been diagnosed in asymptomatic adults as well. Typical xanthomas occur most prominently in the extensor tendons of the hands and Achilles tendon, but can occur in the knees, elbows and buttocks. Xanthomas have been reported in children as young as one to two years of age (25-31). Spinal xanthomas, causing spinal cord compression, have also been reported (32)
The phenotype of sitosterolemia includes abnormal liver function tests, arthralgia, splenomegaly, and hematologic findings (hemolytic anemia, abnormally shaped erythrocytes and large platelets) (33-37). Occasionally, hematologic findings appear as isolated findings (11, 38-41), and there is a case report of an infant with cholestatic jaundice who was ultimately diagnosed with sitosterolemia (42). Aortic stenosis has also been reported (21, 43), as have arthralgias and arthritis (44, 45).
Occasionally, the diagnosis of sitosterolemia is made after an individual with total cholesterol and LDL-cholesterol in the range of familial hypercholesterolemia fails to achieve expected reductions with statin therapy (46). A recent study of 220 hypercholesterolemic children found that 6.4% had elevated and 1.4% had markedly elevated sitosterol levels, with 2 children ultimately diagnosed with genetically confirmed sitosterolemia (47). This has been demonstrated in other publications as well (48, 49). This reaffirms that sitosterolemia is likely underdiagnosed, and high clinical suspicion is warranted. This is particularly important as most genetic testing panels for familial hypercholesterolemia test for pathogenic variants in LDLR, APOB, PCSK9, and LDLRAP1; therefore, individuals with sitosterolemia will frequently have negative genetic testing results.
Although sitosterolemia is a recessive disorder, there is some data suggesting that heterozygous carriers of loss of function mutations can have higher sitosterol levels, higher LDL-cholesterol levels, and a 2-fold higher risk of ASCVD (50).
Differential Diagnosis
Besides sitosterolemia, other disorders that cause tendon xanthomas in children and adults include:
Heterozygous familial hypercholesterolemia (HeFH) - most commonly caused by a co-dominantly inherited disorder of the LDL-C receptor, presents with high total serum and LDL-cholesterol, normal plasma levels of plant sterols and at least one parent with hypercholesterolemia.
Homozygous familial hypercholesterolemia (HoFH) - in which hypercholesterolemia is present in both parents of an affected child. In addition, individuals with HoFH have normal rather than enlarged platelets (macrothrombocytopenia).
Cerebrotendinous xanthomatosis (CTX) - can be distinguished by increased concentrations of plasma cholestanol, protracted diarrhea starting in childhood, and juvenile cataracts. Adults with CTX typically have neurologic involvement (cerebellar ataxia, cognitive decline, and dementia).
Alagille Syndrome, is accompanied by a characteristic syndromic facial appearance, high rates of congenital heart disease, and signs of liver cholestasis (51).
Sitosterolemia should be considered in a child or adult with tendon xanthomas and unexplained hemolysis and/or macrothrombocytopenia, as these hematologic abnormalities are not present in FH, CTX or Alagille syndrome.
Testing
Routine laboratory methods do not always distinguish plant sterols from cholesterol. Detection of plant sterol levels in blood requires gas-liquid chromatography (GLC), gas chromatography/mass spectrometry (GC/MS), or high-pressure liquid chromatography (HPLC).
Plant sterols, especially sitosterol, and the 5-alpha derivatives of plant sterols, are dramatically elevated in patients with sitosterolemia. Plasma concentrations of sitosterol above 1 mg/dL (10µg/mL) are considered to be diagnostic, although a recent study suggested a cutoff value of 15µg/mL had higher positive predictive value (52). Levels typically range from 8-60 mg/dL, 10-25 times higher than normal individuals. Age-dependent reference intervals for phytosterols have also been proposed (53). Molecular genetic testing of mutations in ABCG5 and ABCG8 can help confirm the diagnosis and direct clinical care (54).
In contrast to the very high levels of plant sterols in adults and adolescents with sitosterolemia, total cholesterol levels are sometimes normal or only moderately elevated (34). However, at least three cases of breastfed infants with sitosterolemia presenting with very elevated serum cholesterol levels have been reported. The mechanism of exceptionally high cholesterol levels in sitosterolemic children is unclear (25, 26, 55).
Increased plasma concentrations of plant sterols (especially sitosterol, campesterol, and stigmasterol) are only observed once foods with plant sterols are included in the diet and accumulate in the body. Care must be taken when evaluating infants, since commercial formula feedings with large amounts of vegetable oil may result in elevated sitosterol levels (56).
Children with parenteral nutrition associated cholestasis may have plasma concentrations of plant sterols as high as those seen in patients with hereditary sitosterolemia (i.e., total plant phytosterols of 1.3-1.8 mmol/L). Intralipid typically contains cholesterol, sitosterol, campesterol, and stigmasterol, the latter three of which are plant sterols. Adults receiving parenteral nutrition may also have elevated plasma plant sterol levels (57).
MANAGEMENT OF SITOSTEROLEMIA
Dietary Treatment
Treatment includes dietary restriction of non-cholesterol sterols, limiting intake of shellfish (clams, scallops, oysters), plant foods that contain high fats, such as olives, margarine, nuts, seeds, avocados, and chocolate, and avoidance of vegetable fats and oils (10, 58-61). Fruits, vegetables and cereal products without germ may be used, however (62).
In homozygotes, plasma sterol levels may not improve significantly despite significant dietary sitosterol restriction (63, 64). Margarines and other products containing stanols (e.g., campestanol and sitostanol), which are recommended for use by individuals with hypercholesterolemia, are contraindicated in those with sitosterolemia as they can exacerbate plant stanol accumulation (65).
Medical Treatments
Ezetimibe (Zetia®), inhibits NPC1L1 and decreases the absorption of sterols. It is the first-line drug therapy, lowering plant sterols by 10 to 50% and may stabilize xanthomas (66-69). Hemolytic anemia and platelet abnormalities have been reported to improve as well (66).
Bile acid sequestrants, such as cholestyramine (8-15 g/d), may be considered in those with an incomplete response to ezetimibe(26) Regression of xanthomas has been reported in an 11-year-old after treatment with diet and cholestyramine (70). A 60-year-old man with compound heterozygous mutations in ABCG5 responded to a combination of ezetimibe and alirocumab (71).
Sitosterolemic patients do not have expected clinical responses to statins, which can help to distinguish these patients with elevated plasma sterols and xanthomas from those with familial hypercholesterolemia (64). As stated above, sitosterolemia should be suspected in individuals with hypercholesterolemia who fail to respond as expected to a statin treatment.
Surgical Treatments
Partial ileal bypass surgery (i.e., shortening of the ileum) has been used to increase intestinal bile acid loss. Partial or complete ileal bypass surgery in persons with sitosterolemia has resulted in at least 50% reduction of plasma and cellular sterol and stanol levels (72-74).
Surgical treatments for complications of sitosterolemia have been reported. Liver cirrhosis has been observed at least once in a patient with the ABCG8 mutation. The patient underwent successful treatment by liver transplant, which led to a dramatic improvement in the sitosterolemia. It is possible that restoration of the ABCG8 function in the liver alone may be sufficient to correct the biochemical abnormality (22).
REFERENCES
- 1.
- Gould RG, Jones RJ, LeRoy GV, Wissler RW, Taylor CB. Absorbability of beta-sitosterol in humans. Metabolism. 1969;18(8):652–62. [PubMed: 5799288]
- 2.
- Salen G, Ahrens EH Jr, Grundy SM. Metabolism of beta-sitosterol in man. J Clin Invest. 1970;49(5):952–67. [PMC free article: PMC535768] [PubMed: 5441548]
- 3.
- Salen G, Tint GS, Shefer S, Shore V, Nguyen L. Increased sitosterol absorption is offset by rapid elimination to prevent accumulation in heterozygotes with sitosterolemia. Arterioscler Thromb. 1992;12(5):563–8. [PubMed: 1576118]
- 4.
- Davis HR Jr, Zhu LJ, Hoos LM, Tetzloff G, Maguire M, Liu J, et al. Niemann-Pick C1 Like 1 (NPC1L1) is the intestinal phytosterol and cholesterol transporter and a key modulator of whole-body cholesterol homeostasis. J Biol Chem. 2004;279(32):33586–92. [PubMed: 15173162]
- 5.
- Patel SB, Honda A, Salen G. Sitosterolemia: exclusion of genes involved in reduced cholesterol biosynthesis. J Lipid Res. 1998;39(5):1055–61. [PubMed: 9610773]
- 6.
- Patel SB, Salen G, Hidaka H, Kwiterovich PO, Stalenhoef AF, Miettinen TA, et al. Mapping a gene involved in regulating dietary cholesterol absorption. The sitosterolemia locus is found at chromosome 2p21. The Journal of clinical investigation. 1998;102(5):1041–4. [PMC free article: PMC508970] [PubMed: 9727073]
- 7.
- Patel SB. Plant sterols and stanols: their role in health and disease. J Clin Lipidol. 2008;2(2):S11–S9. [PMC free article: PMC2390824] [PubMed: 19343077]
- 8.
- Berge KE, Tian H, Graf GA, Yu L, Grishin NV, Schultz J, et al. Accumulation of dietary cholesterol in sitosterolemia caused by mutations in adjacent ABC transporters. Science. 2000;290(5497):1771–5. [PubMed: 11099417]
- 9.
- Wang J, Mitsche MA, Lutjohann D, Cohen JC, Xie XS, Hobbs HH. Relative roles of ABCG5/ABCG8 in liver and intestine. J Lipid Res. 2015;56(2):319–30. [PMC free article: PMC4306686] [PubMed: 25378657]
- 10.
- Bhattacharyya AK, Connor WE. β-Sitosterolemia and Xanthomatosis: A NEWLY DESCRIBED LIPID STORAGE DISEASE IN TWO SISTERS. The Journal of Clinical Investigation. 1974;53(4):1033–43. [PMC free article: PMC333088] [PubMed: 4360855]
- 11.
- Escola-Gil JC, Quesada H, Julve J, Martin-Campos JM, Cedo L, Blanco-Vaca F. Sitosterolemia: diagnosis, investigation, and management. Current atherosclerosis reports. 2014;16(7):424. [PubMed: 24821603]
- 12.
- Beaty TH, Kwiterovich PO Jr, Khoury MJ, White S, Bachorik PS, Smith HH, et al. Genetic analysis of plasma sitosterol, apoprotein B, and lipoproteins in a large Amish pedigree with sitosterolemia. Am J Hum Genet. 1986;38(4):492–504. [PMC free article: PMC1684791] [PubMed: 3706300]
- 13.
- Lee MH, Lu K, Patel SB. Genetic basis of sitosterolemia. Curr Opin Lipidol. 2001;12(2):141–9. [PMC free article: PMC1350992] [PubMed: 11264985]
- 14.
- Kidambi S, Patel SB. Sitosterolaemia: pathophysiology, clinical presentation and laboratory diagnosis. J Clin Pathol. 2008;61(5):588–94. [PubMed: 18441155]
- 15.
- Patil S, Kharge J, Bagi V, Ramalingam R. Tendon xanthomas as indicators of atherosclerotic burden on coronary arteries. Indian Heart J. 2013;65(4):491–2. [PMC free article: PMC3860789] [PubMed: 23993019]
- 16.
- Salen G, Horak I, Rothkopf M, Cohen JL, Speck J, Tint GS, et al. Lethal atherosclerosis associated with abnormal plasma and tissue sterol composition in sitosterolemia with xanthomatosis. J Lipid Res. 1985;26(9):1126–33. [PubMed: 4067433]
- 17.
- Bhattacharyya AK, Connor WE, Lin DS, McMurry MM, Shulman RS. Sluggish sitosterol turnover and hepatic failure to excrete sitosterol into bile cause expansion of body pool of sitosterol in patients with sitosterolemia and xanthomatosis. Arterioscler Thromb. 1991;11(5):1287–94. [PubMed: 1911714]
- 18.
- Kolovou G, Voudris V, Drogari E, Palatianos G, Cokkinos DV. Coronary bypass grafts in a young girl with sitosterolemia. Eur Heart J. 1996;17(6):965–6. [PubMed: 8781841]
- 19.
- Hansel B, Carrie A, Brun-Druc N, Leclert G, Chantepie S, Coiffard AS, et al. Premature atherosclerosis is not systematic in phytosterolemic patients: severe hypercholesterolemia as a confounding factor in five subjects. Atherosclerosis. 2014;234(1):162–8. [PubMed: 24657386]
- 20.
- Mymin D, Salen G, Triggs-Raine B, Waggoner DJ, Dembinski T, Hatch GM. The natural history of phytosterolemia: Observations on its homeostasis. Atherosclerosis. 2018;269:122–8. [PubMed: 29353227]
- 21.
- Wang J, Joy T, Mymin D, Frohlich J, Hegele RA. Phenotypic heterogeneity of sitosterolemia. J Lipid Res. 2004;45(12):2361–7. [PubMed: 15375183]
- 22.
- Miettinen TA, Klett EL, Gylling H, Isoniemi H, Patel SB. Liver transplantation in a patient with sitosterolemia and cirrhosis. Gastroenterology. 2006;130(2):542–7. [PMC free article: PMC1391914] [PubMed: 16472606]
- 23.
- Yamamoto T, Matsuda J, Dateki S, Ouchi K, Fujimoto W. Numerous intertriginous xanthomas in infant: A diagnostic clue for sitosterolemia. The Journal of Dermatology. 2016;43(11):1340–4. [PubMed: 27401767]
- 24.
- Peterson AL, DeLine J, Korcarz CE, Dodge AM, Stein JH. Phenotypic Variability in Atherosclerosis Burden in an Old-Order Amish Family With Homozygous Sitosterolemia. JACC: Case Reports. 2020;2(4):646–50. [PMC free article: PMC8298554] [PubMed: 34317312]
- 25.
- Park JH, Chung IH, Kim DH, Choi MH, Garg A, Yoo EG. Sitosterolemia presenting with severe hypercholesterolemia and intertriginous xanthomas in a breastfed infant: case report and brief review. J Clin Endocrinol Metab. 2014;99(5):1512–8. [PubMed: 24423340]
- 26.
- Niu DM, Chong KW, Hsu JH, Wu TJ, Yu HC, Huang CH, et al. Clinical observations, molecular genetic analysis, and treatment of sitosterolemia in infants and children. Journal of inherited metabolic disease. 2010;33(4):437–43. [PubMed: 20521169]
- 27.
- Shulman RS, Bhattacharyya AK, Connor WE, Fredrickson DS. β-Sitosterolemia and Xanthomatosis. New England Journal of Medicine. 1976;294(9):482–3. [PubMed: 1246333]
- 28.
- Davidson CS. The Metabolic Basis of Inherited Disease. Fifth Edition. Edited by John B. Stanbury, James B. Wyn-gaarden, Donald S. Fredrickson, Joseph L. Goldstein, and Michael S. Brown, xvi + 2,032 pp. New York: McGraw-Hill, 1983. Hepatology. 1983;3(3):461-2.
- 29.
- Kalter H. The metabolic basis of inherited disease. 3rd Ed. J. B. Stanbury, J. B. Wyngaarden, and D. S. Fredrickson, eds. McGraw-Hill, New York. 1778 pp. 1972. Teratology. 1972;6(3):362-.
- 30.
- Hubacek JA, Berge KE, Cohen JC, Hobbs HH. Mutations in ATP-cassette binding proteins G5 (ABCG5) and G8 (ABCG8) causing sitosterolemia. Hum Mutat. 2001;18(4):359–60. [PubMed: 11668628]
- 31.
- Watts GF, Mitchell WD. Clinical and metabolic findings in a patient with phytosterolaemia. Ann Clin Biochem. 1992;29(Pt 2):231–6. [PubMed: 1626933]
- 32.
- Hidaka H, Yasuda H, Kobayashi M, Hatanaka I, Takahashi M, Matsumoto K, et al. Familial spinal xanthomatosis with sitosterolemia. Intern Med. 1992;31(8):1038–42. [PubMed: 1477463]
- 33.
- Salen G, Shefer S, Nguyen L, Ness GC, Tint GS, Shore V. Sitosterolemia. J Lipid Res. 1992;33(7):945–55. [PubMed: 1431587]
- 34.
- Björkhem I, Boberg KM, Leitersdorf E. Inborn Errors in Bile Acid Biosynthesis and Storage of Sterols Other than Cholesterol. In: Valle D, Antonarakis S, Ballabio A, Beaudet A, Mitchell GA, editors. The Online Metabolic and Molecular Bases of Inherited Disease. New York, NY: McGraw-Hill Education; 2019.
- 35.
- Salen G, Patel S, Batta AK. Sitosterolemia. Cardiovasc Drug Rev. 2002;20(4):255–70. [PubMed: 12481199]
- 36.
- Su Y, Wang Z, Yang H, Cao L, Liu F, Bai X, et al. Clinical and molecular genetic analysis of a family with sitosterolemia and co-existing erythrocyte and platelet abnormalities. Haematologica. 2006;91(10):1392–5. [PubMed: 17018391]
- 37.
- Wang G, Wang Z, Liang J, Cao L, Bai X, Ruan C. A phytosterolemia patient presenting exclusively with macrothrombocytopenia and stomatocytic hemolysis. Acta Haematol. 2011;126(2):95–8. [PubMed: 21576934]
- 38.
- Kaya Z, Niu DM, Yorulmaz A, Tekin A, Gursel T. A novel mutation of ABCG5 gene in a Turkish boy with phytosterolemia presenting with macrotrombocytopenia and stomatocytosis. Pediatr Blood Cancer. 2014;61(8):1457–9. [PubMed: 24623560]
- 39.
- Wang Z, Cao L, Su Y, Wang G, Wang R, Yu Z, et al. Specific macrothrombocytopenia/hemolytic anemia associated with sitosterolemia. Am J Hematol. 2014;89(3):320–4. [PubMed: 24166850]
- 40.
- Gülen H, Yıldırım AT, Yiğit Y, Yorulmaz A. Typical hematological findings facilitating the diagnosis of sitosterolemia. Pediatr Int. 2021;63(4):472–3. [PubMed: 33881213]
- 41.
- Gok V, Tada H, Ensar Dogan M, Alakus Sari U, Aslan K, Ozcan A, et al. A teenager boy with a novel variant of Sitosterolemia presented with pancytopenia. Clin Chim Acta. 2022;529:61–6. [PubMed: 35167844]
- 42.
- Mandato C, Siano MA, Nazzaro L, Gelzo M, Francalanci P, Rizzo F, et al. A ZFYVE19 gene mutation associated with neonatal cholestasis and cilia dysfunction: case report with a novel pathogenic variant. Orphanet J Rare Dis. 2021;16(1):179. [PMC free article: PMC8048179] [PubMed: 33853651]
- 43.
- Wang Y, Guo YL, Dong QT, Li JJ. Severe aortic valve stenosis in a 14-year-old boy with sitosterolemia. J Clin Lipidol. 2018 [PubMed: 30528907]
- 44.
- Xia Y, Duan Y, Zheng W, Liang L, Zhang H, Luo X, et al. Clinical, genetic profile and therapy evaluation of 55 children and 5 adults with sitosterolemia. J Clin Lipidol. 2022;16(1):40–51. [PubMed: 34969652]
- 45.
- Tada H, Kojima N, Yamagami K, Takamura M, Kawashiri MA. Clinical and genetic features of sitosterolemia in Japan. Clin Chim Acta. 2022;530:39–44. [PubMed: 35248527]
- 46.
- Kiss S, Lee JY, Pitt J, MacGregor D, Wallace J, Marty M, et al. Dig deeper when it does not make sense: Juvenile xanthomas due to sitosterolemia. JIMD Rep. 2020;56(1):34–9. [PMC free article: PMC7653237] [PubMed: 33204594]
- 47.
- Lee JH, Song DY, Jun SH, Song SH, Shin CH, Ki CS, et al. High prevalence of increased sitosterol levels in hypercholesterolemic children suggest underestimation of sitosterolemia incidence. PLoS One. 2020;15(8):e0238079. [PMC free article: PMC7449458] [PubMed: 32845916]
- 48.
- Tada H, Okada H, Nomura A, Yashiro S, Nohara A, Ishigaki Y, et al. Rare and Deleterious Mutations in ABCG5/ABCG8 Genes Contribute to Mimicking and Worsening of Familial Hypercholesterolemia Phenotype. Circ J. 2019;83(9):1917–24. [PubMed: 31327807]
- 49.
- Tada MT, Rocha VZ, Lima IR, Oliveira TGM, Chacra AP, Miname MH, et al. Screening of ABCG5 and ABCG8 Genes for Sitosterolemia in a Familial Hypercholesterolemia Cascade Screening Program. Circ Genom Precis Med. 2022;15(3):e003390. [PubMed: 35549507]
- 50.
- Nomura A, Emdin CA, Won HH, Peloso GM, Natarajan P, Ardissino D, et al. Heterozygous ATP-binding Cassette Transporter G5 Gene Deficiency and Risk of Coronary Artery Disease. Circulation: Genomic and Precision Medicine. 2020;13(5):417–423. [PMC free article: PMC7983048] [PubMed: 32862661]
- 51.
- Alagille D, Odievre M, Gautier M, Dommergues JP. Hepatic ductular hypoplasia associated with characteristic facies, vertebral malformations, retarded physical, mental, and sexual development, and cardiac murmur. J Pediatr. 1975;86(1):63–71. [PubMed: 803282]
- 52.
- Kojima N, Tada H, Usui S, Sakata K, Hayashi K, Nohara A, et al. Serum sitosterol level predicting ABCG5 or ABCG8 genetic mutations. Clin Chim Acta. 2020;507:11–6. [PubMed: 32275988]
- 53.
- Wu M, Pei Z, Sun W, Wu H, Sun Y, Wu B, et al. Age-related reference intervals for serum phytosterols in children by gas chromatography-mass spectrometry and its application in diagnosing sitosterolemia. Clin Chim Acta. 2023;540:117234. [PubMed: 36708942]
- 54.
- Brown EE, Sturm AC, Cuchel M, Braun LT, Duell PB, Underberg JA, et al. Genetic testing in dyslipidemia: A scientific statement from the National Lipid Association. J Clin Lipidol. 2020;14(4):398–413. [PubMed: 32507592]
- 55.
- Rios J, Stein E, Shendure J, Hobbs HH, Cohen JC. Identification by whole-genome resequencing of gene defect responsible for severe hypercholesterolemia. Hum Mol Genet. 2010;19(22):4313–8. [PMC free article: PMC2957323] [PubMed: 20719861]
- 56.
- Hamdan IJA, Sanchez-Siles LM, Garcia-Llatas G, Lagarda MJ. Sterols in Infant Formulas: A Bioaccessibility Study. Journal of Agricultural and Food Chemistry. 2018;66(6):1377–85. [PubMed: 29369630]
- 57.
- Llop JM, Virgili N, Moreno-Villares JM, Garcia-Peris P, Serrano T, Forga M, et al. Phytosterolemia in parenteral nutrition patients: implications for liver disease development. Nutrition. 2008;24(11-12):1145–52. [PubMed: 18656327]
- 58.
- Kratz M, Kannenberg F, Gramenz E, Berning B, Trautwein E, Assmann G, et al. Similar serum plant sterol responses of human subjects heterozygous for a mutation causing sitosterolemia and controls to diets enriched in plant sterols or stanols. Eur J Clin Nutr. 2007;61(7):896–905. [PubMed: 17228349]
- 59.
- Myrie SB, Mymin D, Triggs-Raine B, Jones PJ. Serum lipids, plant sterols, and cholesterol kinetic responses to plant sterol supplementation in phytosterolemia heterozygotes and control individuals. Am J Clin Nutr. 2012;95(4):837–44. [PMC free article: PMC3302361] [PubMed: 22378727]
- 60.
- Gregg RE, Connor WE, Lin DS, Brewer HB Jr. Abnormal metabolism of shellfish sterols in a patient with sitosterolemia and xanthomatosis. The Journal of Clinical Investigation. 1986;77(6):1864–72. [PMC free article: PMC370545] [PubMed: 3711338]
- 61.
- Parsons HG, Jamal R, Baylis B, Dias VC, Roncari D. A marked and sustained reduction in LDL sterols by diet and cholestyramine in beta-sitosterolemia. Clin Invest Med. 1995;18(5):389–400. [PubMed: 8529322]
- 62.
- Tsubakio-Yamamoto K, Nishida M, Nakagawa-Toyama Y, Masuda D, Ohama T, Yamashita S. Current Therapy for Patients with Sitosterolemia --Effect of Ezetimibe on Plant Sterol Metabolism. Journal of atherosclerosis and thrombosis. 2010;17(9):891–900. [PubMed: 20543520]
- 63.
- Cobb MM, Salen G, Tint GS. Comparative effect of dietary sitosterol on plasma sterols and cholesterol and bile acid synthesis in a sitosterolemic homozygote and heterozygote subject. J Am Coll Nutr. 1997;16(6):605–13. [PubMed: 9430090]
- 64.
- Nguyen LB, Cobb M, Shefer S, Salen G, Ness GC, Tint GS. Regulation of cholesterol biosynthesis in sitosterolemia: effects of lovastatin, cholestyramine, and dietary sterol restriction. J Lipid Res. 1991;32(12):1941–8. [PubMed: 1816322]
- 65.
- Connor WE, Lin DS, Pappu AS, Frohlich J, Gerhard G. Dietary sitostanol and campestanol: accumulation in the blood of humans with sitosterolemia and xanthomatosis and in rat tissues. Lipids. 2005;40(9):919–23. [PubMed: 16331855]
- 66.
- Othman RA, Myrie SB, Mymin D, Merkens LS, Roullet JB, Steiner RD, et al. Ezetimibe reduces plant sterol accumulation and favorably increases platelet count in sitosterolemia. J Pediatr. 2015;166(1):125–31. [PMC free article: PMC4274192] [PubMed: 25444527]
- 67.
- Salen G, von Bergmann K, Lutjohann D, Kwiterovich P, Kane J, Patel SB, et al. Ezetimibe effectively reduces plasma plant sterols in patients with sitosterolemia. Circulation. 2004;109(8):966–71. [PMC free article: PMC1237008] [PubMed: 14769702]
- 68.
- Lutjohann D, von Bergmann K, Sirah W, Macdonell G, Johnson-Levonas AO, Shah A, et al. Long-term efficacy and safety of ezetimibe 10 mg in patients with homozygous sitosterolemia: a 2-year, open-label extension study. Int J Clin Pract. 2008;62(10):1499–510. [PubMed: 18822021]
- 69.
- Salen G, Starc T, Sisk CM, Patel SB. Intestinal cholesterol absorption inhibitor ezetimibe added to cholestyramine for sitosterolemia and xanthomatosis. Gastroenterology. 2006;130(6):1853–7. [PubMed: 16697747]
- 70.
- Belamarich PF, Deckelbaum RJ, Starc TJ, Dobrin BE, Tint GS, Salen G. Response to diet and cholestyramine in a patient with sitosterolemia. Pediatrics. 1990;86(6):977–81. [PubMed: 2251034]
- 71.
- Tanaka H, Watanabe Y, Hirano S, Tada H, Nomura A, Kawashiri MA, et al. Sitosterolemia Exhibiting Severe Hypercholesterolemia with Tendon Xanthomas Due to Compound Heterozygous ABCG5 Gene Mutations Treated with Ezetimibe and Alirocumab. Intern Med. 2020;59(23):3033–7. [PMC free article: PMC7759703] [PubMed: 32713907]
- 72.
- Nguyen LB, Shefer S, Salen G, Horak I, Tint GS, McNamara DJ. The effect of abnormal plasma and cellular sterol content and composition on low density lipoprotein uptake and degradation by monocytes and lymphocytes in sitosterolemia with xanthomatosis. Metabolism. 1988;37(4):346–51. [PubMed: 3357417]
- 73.
- Nguyen LB, Shefer S, Salen G, Ness GC, Tint GS, Zaki FG, et al. A molecular defect in hepatic cholesterol biosynthesis in sitosterolemia with xanthomatosis. The Journal of Clinical Investigation. 1990;86(3):923–31. [PMC free article: PMC296812] [PubMed: 2394840]
- 74.
- Salen G, Batta AK, Tint GS, Shefer S, Ness GC. Inverse relationship between plasma cholestanol concentrations and bile acid synthesis in sitosterolemia. J Lipid Res. 1994;35(10):1878–87. [PubMed: 7852865]
- Screening of ABCG5 and ABCG8 Genes for Sitosterolemia in a Familial Hypercholesterolemia Cascade Screening Program.[Circ Genom Precis Med. 2022]Screening of ABCG5 and ABCG8 Genes for Sitosterolemia in a Familial Hypercholesterolemia Cascade Screening Program.Tada MT, Rocha VZ, Lima IR, Oliveira TGM, Chacra AP, Miname MH, Nunes VS, Nakandakare ER, Costa Gurgel Castelo MH, Jannes CE, et al. Circ Genom Precis Med. 2022 Jun; 15(3):e003390. Epub 2022 May 12.
- Heterozygous ABCG5 Gene Deficiency and Risk of Coronary Artery Disease.[Circ Genom Precis Med. 2020]Heterozygous ABCG5 Gene Deficiency and Risk of Coronary Artery Disease.Nomura A, Emdin CA, Won HH, Peloso GM, Natarajan P, Ardissino D, Danesh J, Schunkert H, Correa A, Bown MJ, et al. Circ Genom Precis Med. 2020 Oct; 13(5):417-423. Epub 2020 Aug 30.
- A mouse model of sitosterolemia: absence of Abcg8/sterolin-2 results in failure to secrete biliary cholesterol.[BMC Med. 2004]A mouse model of sitosterolemia: absence of Abcg8/sterolin-2 results in failure to secrete biliary cholesterol.Klett EL, Lu K, Kosters A, Vink E, Lee MH, Altenburg M, Shefer S, Batta AK, Yu H, Chen J, et al. BMC Med. 2004 Mar 24; 2:5. Epub 2004 Mar 24.
- Review Update on Sitosterolemia and Atherosclerosis.[Curr Atheroscler Rep. 2023]Review Update on Sitosterolemia and Atherosclerosis.Rocha VZ, Tada MT, Chacra APM, Miname MH, Mizuta MH. Curr Atheroscler Rep. 2023 May; 25(5):181-187. Epub 2023 Mar 10.
- Review Sitosterolemia: a review and update of pathophysiology, clinical spectrum, diagnosis, and management.[Ann Pediatr Endocrinol Metab. ...]Review Sitosterolemia: a review and update of pathophysiology, clinical spectrum, diagnosis, and management.Yoo EG. Ann Pediatr Endocrinol Metab. 2016 Mar; 21(1):7-14. Epub 2016 Mar 31.
- Sitosterolemia - EndotextSitosterolemia - Endotext
- Nocardiopsis dassonvillei strain AeTV13 16S ribosomal RNA gene, partial sequenceNocardiopsis dassonvillei strain AeTV13 16S ribosomal RNA gene, partial sequencegi|1390220559|gb|MF162276.1|Nucleotide
- Taxonomy Links for Protein (Select 194376618) (1)Taxonomy
- hypothetical protein SY83_03015 [Paenibacillus swuensis]hypothetical protein SY83_03015 [Paenibacillus swuensis]gi|1028462537|gnl|PRJNA272872|SY83_ |gb|ANE45460.1|Protein
- KI-26\w (84)PMC
Your browsing activity is empty.
Activity recording is turned off.
See more...