

NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
Center for Substance Abuse Treatment. Substance Abuse: Clinical Issues in Intensive Outpatient Treatment. Rockville (MD): Substance Abuse and Mental Health Services Administration (US); 2006. (Treatment Improvement Protocol (TIP) Series, No. 47.)
Substance Abuse: Clinical Issues in Intensive Outpatient Treatment.
Show detailsSubstance use disorders exist within several social contexts, one of which is the family. Family members, whether they are from the family of origin or family of choice, are important forces in a client's life. Each client has a family, a family history, and a family story that play important roles in recovery. Many clients come from substance-using families and have been raised with alcohol abuse or drug use as part of their lives. Addressing this legacy is part of their recovery. In addition, a client's family members often have significant substance use and other psychiatric problems of their own. Intensive outpatient treatment (IOT) programs that take a comprehensive approach to evaluating the family are likely to identify other individuals who would benefit from being admitted to a substance abuse or mental health treatment program. Some family members may be in treatment already. For these reasons, many IOT programs incorporate a family systems approach. Family education, family therapy, and other services are necessary in an IOT program's process so that the contributions and influence of family members support recovery.
A complete discussion of family therapy for substance use disorders in IOT programs is not within the scope of this TIP. This chapter introduces features of family involvement in IOT programs and briefly discusses family therapy as an enhanced service that IOT programs may offer or, more frequently, to which they may refer clients and their families. The Center for Substance Abuse Treatment has developed TIP 39, Substance Abuse Treatment and Family Therapy (CSAT 2004c ), that addresses how a substance use disorder affects the family, how family therapy works to change the interactions among family members, and the integration of family therapy into substance abuse treatment.
Families of people who abuse substances live in a world shaped by substance use. This world may include inconsistent behaviors and few or very rigid rules. Family members may have difficulty expressing their emotions, achieving intimacy, and solving problems. They frequently may experience but may not express anger, shame, guilt, sadness, and hopelessness. To function, families often subscribe to the following: don't trust, don't feel, and don't talk. The result can be an unhealthy environment in which individuals may be isolated, engage in destructive alliances, be overly involved with other family members, or develop significant medical and stress-related problems.
Increasingly, treatment professionals view substance use disorders from a family systems perspective (Crnkovic and DelCampo 1998). Research findings document a relationship between family involvement in treatment and positive outcomes and attest to the need for family-based services (Rowe and Liddle 2003). Family involvement in treatment seems to work equally well for adults and adolescents (Stanton and Shadish 1997). When the family is ready and able to shift from old, negative behaviors to new, healthier ones, family members become collaborators in the treatment process (Edwards and Steinglass 1995). Most IOT programs do not offer couples- or family-based therapies (Fals-Stewart and Birchler 2001). However, potential benefits of family therapy are such that IOT programs should have well-established links with organizations that provide these services.
No matter how alienated family members may be, they are critical to the strength and duration of the client's recovery. Family members are the individuals who were part of the client's life before treatment and will be part of his or her life after treatment. Family-based services that are part of IOT help ensure that family functioning adjusts to and positively influences the recovery of the client.
Planning for Family Involvement
IOT planning for family-based services involves defining the client's family in broad and flexible terms, setting essential goals, and determining the desired outcomes.
Defining the Family
In recent years, the concept and definition of family have broadened significantly to include people who are important to the client. These people can include a spouse, a boyfriend or girlfriend, a same-sex partner, parents, siblings, children, extended family members, friends, co-workers, employers, members of the clergy, and others. The term “family of origin” commonly is used to describe individuals related by blood, such as parents, grandparents, and siblings. The term “family of choice” is used to describe a family created by marriage, partnership, or friendships and other associations.
When determining the client's concept of family, the key is to identify who will be supportive of recovery and who might seek to undermine it. The treatment provider can begin this process by creating a genogram (see appendix 6-A) to assess the family of origin or choice. Similarly, a social network map (see appendix 6-B) can help the counselor identify and understand the family of origin and family of choice.
- Creating a family genogram. This technique renders the client's family relationships schematically and helps the counselor identify trends or patterns in the family history and understand the client's current situation. As treatment progresses, the genogram is revised to reflect new knowledge and changes in the family (CSAT 2004c ).
- Assessing the client's social supports with a social network map. A social network map displays the links among individuals who have a common bond, shared social status, similar or shared functions, or geographic or cultural connection. Highly flexible, social networks form and disband on an ad hoc basis depending on specific need and interest. A social network assessment is used in social service arenas, including substance abuse treatment. When the assessment is used in IOT, individuals are identified who can support the client or participate in the treatment process (Barker 1999).
Goals and Outcomes of Family Services
One main goal of involving families in treatment is to increase family members' understanding of the client's substance use disorder as a chronic disease with related psychosocial components. Edwards (1990) states that family-based services can have the following effects:
- Increase family support for the client's recovery. Family sessions can increase a client's motivation for recovery, especially as the family realizes that the client's substance use disorder is intertwined with problems in the family.
- Identify and support change of family patterns that work against recovery. Relationship patterns among family members can work against recovery by supporting the client's substance use, family conflicts, and inappropriate coalitions.
- Prepare family members for what to expect in early recovery. Family members unrealistically may expect all problems to dissipate quickly, increasing the likelihood of disappointment and decreasing the likelihood of helpful support for the client's recovery.
- Educate the family about relapse warning signs. Family members who understand warning signs can help prevent the client's relapses.
- Help family members understand the causes and effects of substance use disorders from a family perspective. Most family members do not understand how substance use disorders develop or that patterns of behavior and interaction have developed in response to the substance-related behavior of the family member who is in treatment. It is valuable for individuals in the family to gain insight into how they may be maintaining the family's dysfunction. Counselors should help family members address feelings of anger, shame, and guilt and resolve issues relating to trust and intimacy.
- Take advantage of family strengths. Family members who demonstrate positive attitudes and supportive behaviors encourage the client's recovery. It is important to identify and build on strengths to support positive change.
- Encourage family members to obtain long-term support. As the client begins to recover, family members need to take responsibility for their own emotional, physical, and spiritual recovery.
A comprehensive IOT program views the client as part of a family system. When the family is involved in treatment, the following treatment outcomes are possible:
- The client is encouraged to enter treatment.
- The client is motivated to remain in treatment.
- Relapses are minimized.
- A supportive and healthy environment for recovery is provided.
- Other family members who may need treatment or other services are identified and treated.
- Changes in the family's longstanding dysfunctional patterns of communication, behavior, and emotional expression may protect other family members from abusing substances.
Engaging the Family in Treatment
Difficulties with engaging the family in treatment often are cited as reasons for not using a family systems approach and, in many cases, substantial obstacles exist. Family members may be resistant, or the client may be ambivalent or object to the family's involvement in treatment. But given the potential benefits associated with taking a family approach to service delivery, engaging the family in treatment is worthwhile.
Strategies To Engage the Family
The following approaches have proved helpful in encouraging families to engage in the treatment of a family member:
- Include family members in the intake session. The counselor can involve family members in the treatment process from the beginning. If a family member makes the initial call to the program, the counselor can ask that person to come with the client. If the client calls, the client can be asked to bring a family member. If the client is reluctant at this point, the counselor can gently encourage the client to include family members but should not make it a condition of the person's entry into treatment. In another approach, the counselor can ask, “Who close to you is concerned about your substance use and might be willing to serve as a support to you during your recovery?” The client then might be asked to invite these supportive people to come to the initial intake interview. During the intake interview, family members can be asked to complete a brief written family assessment. A more comprehensive family systems approach can involve multiple private and family interviews. These interviews and other early meetings with the family develop support from a family that is empowered to address systemic issues. Similarly, the initial meeting helps family members learn about substance use disorders, their influence on a family, and the services the program can offer to the family (see Exhibit 6-1).
Exhibit 6-1. Suggestions for Engaging Family Members at Intake
Emphasize the need to gather information from family members. State the program's policy about family members' participation in treatment. Indicate the program's desire to hear family members' concerns about the client's substance abuse. Acknowledge family members' influence over the client and their desire to help. Make clear that family members' participation will help the client on the road to recovery. Emphasize how the program can help family members maintain a relationship with the client and manage their own feelings (anger, frustration, depression, and hopelessness). - Use client-initiated engagement efforts. The counselor and client collaborate on a plan to engage family members in treatment. The client can be given the opportunity to invite chosen family members to participate in the program. If this effort is unsuccessful, then, with the client's written permission, the counselor telephones, visits, or sends a personal note to the identified family members. Federal confidentiality rules require that client permission be documented (CSAT 2004b ).
- Offer a written invitation. The IOT provider can give the client written invitations, with the clinic's contact information, to deliver to family members. Giving the client the invitations allows the provider to determine whether the client is willing to involve family members in treatment and which family members the client wants to involve in the process. The invitation briefly describes the treatment program and identifies activities family members will be asked to participate in. For example, a family member may be asked to attend family education sessions, complete an assessment questionnaire, remove all substances from the home (if applicable), participate in family counseling sessions, or attend a celebration of the completion of a treatment phase.
- Offer incentives. Incentives may help address recruitment problems. Family members can be provided with coupons (e.g., for pizza, movies) for attending sessions or completing assignments. Refreshments also help family members feel welcome. In addition, providers can facilitate transportation (e.g., arrange carpools) and childcare services and remove other obstacles to family members' participation.
- Plan picnics or dinners for families. Multifamily picnics and dinners are a part of some IOT programs and can be scheduled for holidays or weekends. These events can be held on the program's grounds or in nearby parks or community centers and provide a supportive and nonthreatening environment where individuals can have fun and learn about substance use disorders, recovery, and the IOT program. The client and family members are asked to bring a dish, but all are welcome. Immediately after the meal, a counselor conducts an hour-long educational session covering topics such as recovery support groups, family-oriented services, and characteristics of substance use disorders. Participants are told of the educational nature of the sessions when invited.
- Use community reinforcement training (CRT) interventions. CRT interventions have improved the retention of family members in treatment and induced people who abuse substances to enter treatment (Meyers et al. 1998, 2002). Among other strategies, the CRT approach teaches family members that substance abuse is not a moral failing but a disease and that they are not the cause of and cannot be the cure of their loved one's substance use disorder. They also learn to identify and pursue their own interests, communicate in nonjudgmental ways, encourage drinking of nonalcoholic beverages during social occasions, manage dangerous situations, and discuss treatment entry with the family member who abuses substances when the consequences of abuse are severe (Kirby et al. 1999b ).
- Use the resources of the program. To create a family-friendly environment, IOT staff at all program levels need to work together toward the goal of engaging families. For example, flexible program hours and large offices or meeting rooms may be needed to accommodate family schedules and large families. Safe toys should be made available for children so that they are less likely to disrupt a session. Front office staff should be trained to encourage and reinforce the efforts of family members who call or come in with the client for the initial visit. Programs can organize their client record systems and procedures so that staff members have easier access to family-related information for each client.
- Provide a safe, welcoming environment. Family members may be anxious or reluctant to participate in the treatment process. A welcoming environment encourages them to participate despite their concerns. A safe, clean, and cheerful meeting space is important. Good lighting, a well-marked and well-maintained exterior, culturally appropriate décor, comfortable furniture, and amusements for children convey the message that family members are welcome, valued by the treatment team, and essential to the recovery of the client. Ice-breaking activities, simple games, and role-play activities can make the group meeting inviting and encourage family involvement.
Overcoming Barriers to Engaging Family Members in Treatment
Not all family members participate in the treatment process. Sometimes individuals are reluctant to become involved with treatment, even though they care about the client. Women are more likely to be involved in their male partners' treatment; men are less likely to participate in their female partners' treatment (Laudet et al. 1999). Also, the client may not want family members to be involved because of threats of domestic violence or past abuse by a family member, guilt about the substance abuse, fear that family secrets may be revealed, concern about adding to the family burden, or other reasons. All family members who do participate must feel free to raise pertinent issues, even if another family member objects. Because of the risk of domestic abuse that comes with raising difficult issues, providers must assess carefully the potential for violence within the family (CSAT 2004c ).
Despite these barriers, the IOT provider is encouraged to take every possible action to engage families of clients in the treatment process. Better client retention, fewer relapses, improved family functioning, and family healing are all possible outcomes (O'Farrell and Fals-Stewart 2001).
Supportive supervision of the counselors providing these family services
- Gives staff members confidence that they are providing appropriate levels of service while addressing clinical issues that inevitably arise
- Ensures that counselors and staff members understand their limitations in working with family members
- Guards against counselors and staff members attempting to provide therapy for which they have not been trained
When working with families, programs can make use of existing partnerships with agencies and groups that provide enhanced family services, individual counseling for other family members, health care, and financial and legal services to support clients' families.
Family Services
Family members
- May need guidance on how to address many issues that can arise during early recovery
- May have questions or misconceptions about substance use disorders
- May need to find healthy ways to handle their justifiable feelings of anger, frustration, shame, helplessness, guilt, and sadness that stem from attempts to fix the client's substance use disorder
- May need the counselor's intervention to understand and avoid behaviors that contribute to the client's continued use of alcohol and drugs
The types of services described in this section can support the efforts of family members as the client moves through the course of treatment. Although every family is different, and the pace of recovery varies from family to family, a sample treatment calendar is provided in Exhibit 6-2. IOT services can assist family members in accomplishing the tasks described in the calendar.
Exhibit 6-2. A Treatment Calendar for Family Members
Beginning stage: 1–5 weeks • Commit to treatment. • Understand that a substance use disorder is a chronic illness. • Support abstinence. • Begin to identify and discontinue behaviors that support substance use. • Learn about the family support groups: • Al-Anon (www .al-anon.alateen.org) • Nar-Anon (www .naranon.com) • Families Anonymous (www .familiesanonymous.org) Middle stage: 6–20 weeks • Assess the relationship with the client. • Develop a realistic perspective on addiction-related behaviors so the family member remains involved with the client but establishes some protective personal distance. • Work to eliminate behaviors that encourage the client's substance use (i.e., enabling behaviors). • Move past behaviors that are primarily a response to the client's substance use (i.e., codependence). • Seek new ways to enrich the family member's life. • Begin practicing new communication methods. Advanced stage: 21+ weeks • Work to develop a healthy, balanced lifestyle that supports the client and addresses personal needs. • Exercise patience with recovery. • Evaluate and accept changes, adaptations, and limitations.
Source: Matrix Center 1989.
Family Education Groups
Family education groups provide information about the nature of a substance use disorder; its effects on the client, the family, and others; the nature of relapse and recovery; and family dynamics. These groups often motivate families to become more involved in treatment.
The family education group typically meets weekly for 2 to 3 hours, often in the evening or on weekends, and includes between 10 and 40 individuals. The group is facilitated by a counselor and usually covers these topics:
- Medical aspects of addiction and dependence
- Relapse and relapse prevention
- Addiction as a family disease
- Subconscious refusal to admit that the client has a substance use disorder (i.e., denial)
- Enabling behaviors
- Communication
- Reasons for testing and monitoring of the client
- Leisure time planning
- Parenting skills
- Community support groups and resources
Group members listen to lectures, discuss topics, and engage in exercises that help them become knowledgeable about substance use disorders and their effects on the family.
Multifamily Groups
Multifamily groups can be thought of as microcosms of the larger community. They offer more opportunities for learning, adaptation, and growth than do groups of one client and family members. These groups provide family members with a sense of normalcy and a support network. Individuals learn that other families face similar difficulties. This discovery may reduce the stigma and shame commonly found among families struggling with substance use disorders. Families often exhibit mutually supportive, spontaneous involvement with one another and reinforce one another's problemsolving approaches. Cross-learning—in which, for example, a man learns to understand his wife better by listening to other husbands and wives—is one of the most powerful effects of multifamily therapy. Incorporating multifamily groups into IOT has been shown to increase the length of treatment for female clients, increase completion rates for men, and improve family functioning and children's behavior (Boylin and Doucette 1997; Meezan and O'Keefe 1998). Treatment providers report that having more than one generation present in the group can help institute a family's commitment to abstinence and recovery (Conner et al. 1998).
Multifamily groups typically engage several clients and their family members in group exercises that teach them how to develop healthy communication techniques, avoid enabling behaviors, reduce codependence, and get help. Until a multifamily group coalesces, it may be helpful for members' participation to be structured (e.g., talking only about themselves, not about the person in IOT).
IOT providers should foster an atmosphere of acceptance and emotional safety so that learning occurs in a relaxed setting. Group sessions generally are scheduled weekly and last for 2 to 4 hours with group size ranging from 12 to 30 members (6 to 8 families) (Crnkovic and DelCampo 1998). Clients' recovery may be aided by the inclusion of supportive individuals from outside the family (e.g., sponsors, friends, religious leaders, co-workers). The consensus panel recommends that multifamily groups be co-led by two therapists trained in this process. Membership may change frequently, and clients and their families join the group as others graduate from the treatment program.
Family Therapy Groups
In 1997, Stanton and Shadish conducted a meta-analysis that compared the effectiveness of family education, family therapy, and other forms of family intervention for people with substance use disorders. Their results suggested family therapy is more effective than family education groups and other family services. However, family therapy can be delivered only by specially trained therapists. Forty-two States require that people practicing as family therapists be licensed. In most States, a family therapist must have a master's degree to practice independently (CSAT 2004c ). Family therapy addresses the dynamics in the family that may encourage substance abuse and offers support for changing these dynamics. It emphasizes that the family as a dynamic system, not merely the inclusion of family members in treatment, is the hallmark of family therapy (CSAT 2004c ). These sessions may include individual family, couples, and child-focused therapy. (Family therapy for adolescents is discussed in chapter 9.) Because not all IOT programs provide these types of therapy groups, providers should consider establishing referral agreements with other community service organizations that provide family therapy.
Individual family therapy
This type of therapy helps family members look at their interactions and identify the factors in the family that contribute to a substance use disorder. Family members are encouraged to restructure negative patterns of behavior and communication into interactions that are more conducive to recovery for everyone. Through family therapy, adults and children express to the client how behavior has affected them and how new coping skills now are affecting their lives. The client has the opportunity to use new skills learned in treatment and to receive constructive feedback from family members in a safe environment. During these sessions, families may address issues such as irresponsible behavior, indebtedness, substance use in the home by other family members, availability of alcohol on special occasions, and how to reveal treatment and recovery to others. The content of these sessions varies significantly, based on the needs and motivations of the family members. Family therapy may be scheduled monthly or more frequently.
Couples therapy
Couples counseling is useful in improving certain aspects of functioning in families with substance use disorders (O'Farrell and Fals-Stewart 2002). This therapy focuses on improving a couple's relationship and reducing problems related to substance abuse. The spouse or significant other is taught to reinforce abstinence, decrease behaviors that cue substance use, and avoid protecting the client from the adverse consequences of substance use. Both partners are taught to increase positive exchanges, improve communication, and work together to solve problems. The number of sessions can be six or more and can include sessions for one couple or groups of couples (Fals-Stewart et al. 1996).
Child-focused therapy
Play and structured recreational activities for children and parents can reduce conflict in families with substance use disorders. In groups with their children, parents are taught parenting and problemsolving skills and are given information about normal childhood development. Parents recovering from substance use disorders have a chance to experience pleasurable recreational activities with their children (e.g., volleyball, soccer) and learn to interact with them in a structured, therapeutic setting. Older children can be educated about substance use and how it can affect them and their families.
Family Retreats
Some IOT providers have found that family retreats can be effective in helping families harmed by substance use disorders, although research is unavailable on this topic. Participants can take important steps toward healing damaged relationships. Some participants have described family retreats as the most important aspect of their experience in treatment.
Most family retreats cover 2 days, usually over a weekend; participants spend nights at home. Retreats provide clients and their family members with the opportunity to work intensively with one another to address powerful emotions such as shame and guilt and to restore lost intimacy and trust. Participants take part in education sessions, exercises, and group activities. Day 1 activities can include family education on
- Communication skills
- Experiencing and working with feelings
- Developing trusting relationships within the family
- Creating healthy expectations
- Reestablishing roles
Participants receive an assignment the evening of day 1 to work on at home. Assignments may focus on developing relapse contracts, reading from journals, or sharing positive family memories. Day 2 can focus on a therapeutic event during which
- Participants discuss the assignments they completed the night before.
- Family members are encouraged to tell one another important things, which may never have been said or discussed before.
- Family sculpting exercises are conducted; this activity dramatically illustrates relationships and communication patterns that need to change. In family sculpting, each family member takes a turn positioning the other family members in relation to one another, posing them as he or she sees fit, and explaining the choices (CSAT 1999a ).
Programs that conduct retreats find that executing a “contract for participation” with the client helps ensure that the retreats are well attended. Therapists may need to assist the client in recruiting family members to attend. Retreats should be staffed by therapists who are experienced in managing highly emotional events.
Support Groups for Families
Mutual-help groups provide the continuing emotional, educational, and interpersonal support that family members often need as clients complete their treatment. Attending support group meetings helps family members adjust to changes being made by the recovering member and begin new lives of their own. Family support groups may be sponsored on an ongoing basis by the IOT program or consist of community-based fellowships such as Al-Anon, Nar-Anon, Alateen, Adult Children of Alcoholics (www.adultchildren.org), Adult Children Anonymous (www.12stepforums.net/acoa.html), and Families Anonymous.
When a family support group is sponsored by the IOT program, it usually meets weekly. Family members can discuss problems and concerns that arise because of the client's recovery and reconnection with the family. Such groups offer continuity for family members during the difficult treatment and recovery periods. Surrounded by familiar program staff members and other family participants, family members build on the momentum of their previous experiences in treatment. Examples of the issues discussed include parenting, decisionmaking, conflicts, sexual functioning, intimacy, anger management, mood swings, reestablishing trust, adjusting roles, learning what is “normal,” renegotiating relapse prevention contracts, and substance use by other family members.
Community-based 12-Step support groups such as Al-Anon, Nar-Anon, and Alateen are independent from the IOT program. Because family members may be reluctant to initiate contact with such groups, IOT providers can assist family members by providing information about meetings, such as what happens at these meetings, the rituals observed, who attends, how meetings are conducted, the purpose of the meetings, and where to find them. Members of mutual-help groups can be invited to give talks to the family members in the IOT program. Providers also should emphasize that the meetings are anonymous. By encouraging family members to attend at least three meetings before deciding whether to continue, the IOT provider increases the probability that family members have a positive experience and continue to attend. IOT staff can encourage members of multiple families from the program to attend meetings together so that they can reinforce and reassure one another.
Family Clinical Issues in IOT
Diverse questions, concerns, and behaviors are presented by family members during IOT sessions. The complexity of human relationships and interactions is revealed in treatment and can challenge both participants and counselors to use the opportunities and experiences therapeutically. Long suppressed anger, family secrets, shame, and confusion may surface. Family members may harbor feelings and thoughts that can affect the client and the family adversely and that require resolution within a therapeutic environment.
Unrealistic Expectations About Treatment Outcomes
Family members often have unrealistic expectations about treatment and the client's recovery. Family members may not understand the nature of a substance use disorder or are unable to accept that it is a chronic, relapsing disease and recovery is a lifelong process. Some family members, for instance, can be so fatigued and emotionally depleted from the stress of living with the person who abuses substances that they have unrealistic hopes for treatment. Strategies and solutions to address unrealistic expectations and common fallacies about treatment and recovery include the following:
- Informing the family early in treatment about common but unrealistic expectations. By gently raising this issue early in treatment during individual family sessions, the IOT counselor can draw attention to and begin to dispel any fallacies. The counselor can probe for related family beliefs, answer family members' specific questions, and provide real-life examples before unrealistic expectations lead to an undermining of family and client functioning. This process also can identify specific educational needs.
- Using a variety of formats to provide clear, understandable information about substance use disorders. A family education group is a basic component of IOT programming that is effective in debunking many fallacies about substance use disorders. For instance, the group can be used to dispel the idea that once a client is in treatment, he or she will stop having the urge to use; that once use stops, everything will be “perfect”; or that doctors and counselors will teach how to get well. A counselor can obtain or develop written materials (fact sheets, brochures, posters) at appropriate reading levels and in relevant languages. These materials need to be available at the program facility and distributed to family members at intake and during treatment. A brief, informative video can be played during family sessions, in counselors' offices, or in the waiting room.
- Reaching many family members. It is important to educate as many family members as possible and to ensure that the most influential family members become knowledgeable about substance use disorders and then redirect other family members if necessary.
Changing Realities: Working With Clients Who Are Estranged From Their Families In one IOT program, some clients revealed that they did not participate in family groups, family nights, and other family-oriented activities because they had no family. The clients had been ostracized by or estranged from family members for an extended period. The counselors suggested that clients and staff rename the “family” events so that clients could feel more comfortable bringing other individuals such as co-workers or friends who made up their family of choice. Instead of Family Night, the program sponsored Support Network Night. The results • Participation in the events increased. More clients and their supporters attended treatment activities. • Clients were encouraged to build an abstinent support network that included friends, co-workers, neighbors, or others as well as members of their family of origin.
Family Responses to Relapse
Clients can relapse, and family members may be unwilling or unable to be compassionate or nonjudgmental about episodes of relapse. Typically, relapse is an unpopular topic with family members. If relapse occurs, counselors need to be prepared for a range of emotional responses from families, including anger, panic, blame, depression, spitefulness, and relief. Some families may abandon or withdraw from the client; others may attempt to engage the client in substance-using activities; still other families may be caught in patterns of depression and resignation or panic and fear.
Living the Treatment Process Anthony's wife and son were relieved and optimistic when he entered treatment. Soon they would be able to enjoy the husband and father they had missed during many years of substance abuse. As the weeks passed, however, Anthony's family grew more angry and disappointed. He rarely spent time with them and was always at recovery meetings. He showed little interest in their lives and was not physically or emotionally available to them. “I thought treatment would make our lives better, but it's just not true,” said his wife. Counselor's response • Validate the feelings of family members. • Explain that Anthony's recovery requires his full attention. For a time, he will be unable to devote much attention to the needs or expectations of others. Only as his recovery progresses and risk of relapse recedes can he become less self-focused. • Discuss the warning signs of relapse. • Emphasize the family members' need to focus on enhancing their own lives, independent of the addicted loved one, including involvement in support groups such as Al-Anon.
The following therapeutic options may help counselors in assisting families that may experience a family member's relapse:
- Prepare the family members as well as the client for the possibility of relapse. Family members are likely to be the first to know when a client relapses. IOT programs focus on strengthening the client's relapse prevention skills, but families also need assistance. IOT staff members can help families
- Understand that relapse can happen and that each family reacts in unique ways.
- Accept that their reactions to the relapse crisis do not necessarily indicate that the family is in deep trouble.
- Prepare a plan that identifies steps the family will take if relapse occurs.
- Identify ways that family members can support one another.
- Seek help if the plan fails.
- Assist family members in engaging support services and resources. Community-based support groups such as Al-Anon, Nar-Anon, Alateen, and Alatot (for children of parents who abuse alcohol) are available in most areas and are indispensable sources of help for many families. Family members should be encouraged to attend meetings regardless of the client's recovery status. In these groups, family members focus on their own needs, accept what they cannot change, and engage in healthy, satisfying activities. To facilitate attendance, some IOT programs offer these groups space at their facility. Others sponsor their own family support groups, led by alumni of the programs, that are open to all who wish to attend for as long as they desire.
- Seek interventions for individual family members when their responses to relapse are unhealthy. The IOT counselor needs to be alert to the possibility that relapse by a client may require additional family interventions and referrals to other service professionals. For example, another family member also may be in recovery and may need additional assistance from a support group. Another family member may become depressed as a result of the client's relapse, or an adolescent may act out. The client and other family members may benefit from psychological or psychiatric interventions.
Sabotage by Family Members
A family can sabotage the client's progress when one or more family members behave in ways that undermine the client's abstinence or treatment. For example, family members may continue to use or leave alcohol or drugs where the client is likely to see them. They may state to the client or others that the client is likely to fail or may refuse to let the client use the family car to go to a support meeting or treatment session. Examples of successful clinical approaches to discourage sabotage and encourage positive participation are as follows:
- Schedule individual family sessions to discuss the specific behaviors that are sabotaging recovery efforts.
- Discuss alternative behaviors that support recovery, and offer support for making the behavioral changes.
- Determine whether individual therapy is needed, and support family members with a referral to a family therapist as appropriate.
- Work with family members to create a contract that specifies how their behavior is to change.
- Monitor progress.
Family Life Without Substance Abuse
As recovery begins, some family problems resolve with abstinence. Issues of trust and worries about how the family will be different are likely to emerge. Here are a few common questions and some suggested answers on how IOT counselors can help families:
- How do we reestablish trust?
- Teach family members that a lack of trust is a normal and natural reaction in early recovery but, at the same time, the recovering person may sense this lack of trust and may become angry or sad.
- Indicate that the newly abstinent member may suffer from a “time warp” in which a week seems more like a month. Such different perceptions of time can add to conflict around the trust issue because the client may expect the family's trust after what is, in reality, only a short period of abstinence.
- Discuss the idea that mistrust transforms into trust only as the client maintains abstinence and demonstrates positive changes in behavior. Ask the client to accept that family members may not trust him or her for a period.
- Suggest that family members agree to extend their trust incrementally to the client. For example, an adolescent client may be given permission to use the family car for an outing if the adolescent's school attendance is satisfactory for a specific period.
- How do we have fun again?
- Suggest creating new family rituals to replace old ones that involved substance use.
- Suggest establishing and celebrating “family” abstinence anniversaries.
- Encourage participation in events sponsored by Al-Anon, Nar-Anon, and other family support groups.
- Urge participation in multifamily groups sponsored by the treatment program.
- Ask each member to identify a favorite “family fun” activity for the entire family to enjoy.
- Ask members to consider separate couples and parent-child activities to create new relationships between family members.
- Ask members to keep a family journal that includes ideas, feedback, and comments from family members on various activities, rituals, and other family events.
- What do we say to friends, neighbors, and associates about treatment and recovery?
- Assist family members in discussing and coming to decisions about what information they want to share with others and when. Write down this information, give it to all family members in the form of an agreement, and have each member sign the agreement.
- Review the privacy and confidentiality provisions that govern treatment programs with family members to remind them that providers will not discuss these topics with others and that family members are in control of what others know. Use family support group sessions to discuss this issue so that members learn from the experiences and examples of other families.
- Have family members “rehearse” situations they are likely to encounter to practice appropriate responses.
- First the bottle, now the meetings. Will it ever get better?
- Acknowledge that the spouse or significant other is disappointed and frustrated.
- Point out that recovery is the first and most important goal during this difficult period and that people in recovery often immerse themselves in recovery activities with the same intensity with which they used substances.
- Assist the spouse or significant other in focusing instead on his or her own recovery and in attending Al-Anon, Nar-Anon, or other support groups.
Appendix 6-A. Format and Symbols for Family Genogram*
The genogram is useful for engaging the client and significant family members in a discussion of important family relationships. Squares and circles identify parents, siblings, and other household members, and an enclosed square or circle identifies the client. Marital status is represented by unique symbols, such as diagonal lines for separation and divorce. Different types of connecting lines reflect the nature of relationships among household members. For instance, one solid line represents a distant relationship between two individuals; three solid lines represent a very close relationship. Other key data, such as arrest information, are written on the genogram as appropriate.
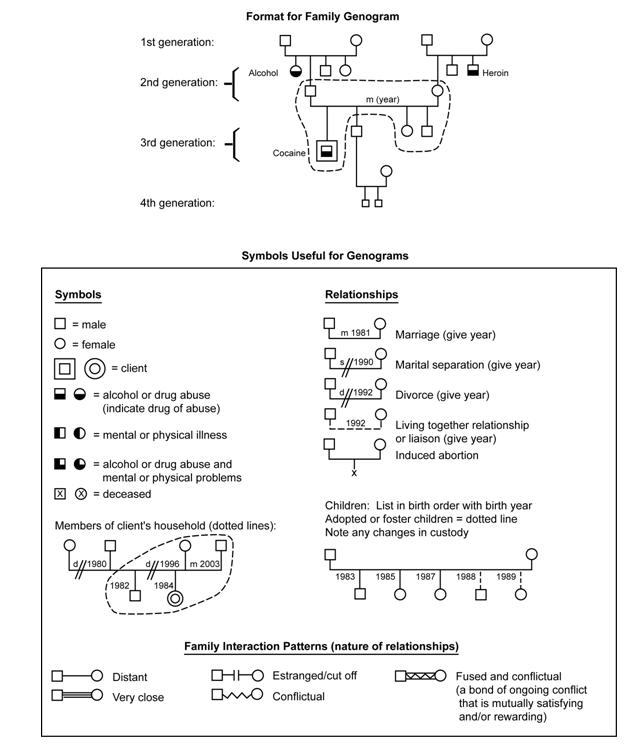
*Source: New Jersey Division of Addiction Services, New Jersey Department of Health and Senior Services.
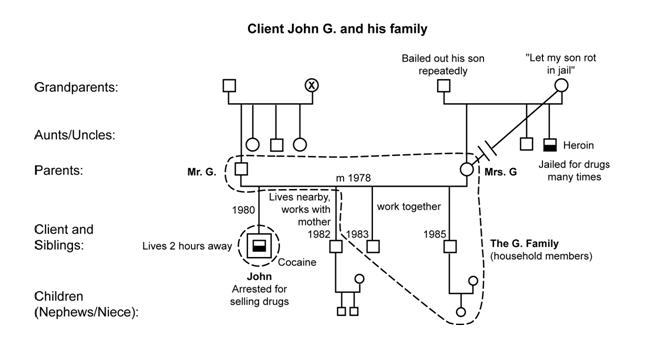
This sample genogram depicts a family that initially was seen as a close, loving family unit. The son, John, had come under the influence of some “bad friends” and had become involved in abusing and selling substances. While expressing their willingness to help, the family denied the seriousness of the situation and minimized any problems in the nuclear or extended family.
When the discussion was extended to one of John's maternal uncles, Mrs. G. admitted that her brother had been arrested a number of times for heroin possession. Questions about the maternal grandmother's reaction to John's “problem” caused the united family front to begin to dissolve. It became apparent that Mrs. G.'s mother took an “insensitive position” regarding John's substance use disorder and there was a serious estrangement between her and her daughter. In discussing the details of the uncle's criminal activity (which was a family secret that even John and his brothers did not know), it emerged that Mrs. G. had for years agonized over her mother's pain. Now, desperately afraid of reliving her parents' experiences, Mrs. G. had stopped talking to her mother. John's brothers felt free to open up and expressed their resentment of their brother for putting the family in this position.
Mr. G., who had been most adamant in denying any family problems, now talked about the sense of betrayal and failure he felt because of John's actions. It was only through the leverage of the family's experience that the family's present conflict became evident.
Source: New Jersey Division of Addiction Services, New Jersey Department of Health and Senior Services.
Appendix 6-B. Family Social Network Map*
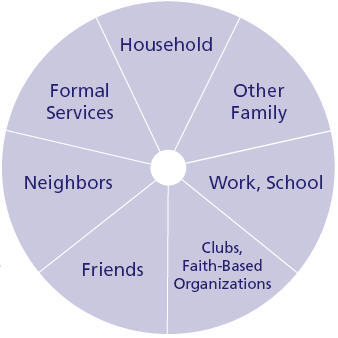
Designing a social network map is a practical strategy to survey various aspects of social support available to clients and their families. Mapping a client's social network is a two-stage process. First, the client uses a segmented circle to categorize people in the network (e.g., friends, neighbors). Then, a grid is used to record a client's specific responses about the supportive or nonsupportive nature of relationships in the network (Tracy and Whittaker 1990). This approach allows both clinicians and clients to evaluate (1) existing informal resources, (2) potential informal resources not currently used by the client, (3) barriers to involving resources in the client's social network, and (4) whether to incorporate particular informal resources in the formal treatment plan. Mapping also can identify substance-using behaviors of individuals in the client's social network. The map takes an average of 20 minutes to complete and provides a concise but comprehensive picture of a family's social network. Practitioners report that the social network map identifies and assesses stressors, strains, and resources within a client's social environment (Tracy and Whittaker 1990). This interactive, visual tool allows clients to become actively engaged and gain new insight into how to find support within their social networks.
Instructions
Step one. Explain to the client that you would like to take a look at who is in the client's social network by putting together a network map. The client can use a first name or initials for each important person in his or her life; either the clinician or the client can enter the names in the appropriate segment of the circle shown below.
Sample script. Think back over this past month, say since [date]. What people have been important to you? They may have been people you saw, talked with, or wrote letters to. This includes people who made you feel good, people who made you feel bad, and others who just played a part in your life. They may be people who had an influence on the way you made decisions during this time.
There is no right or wrong number of people to identify. Right now, just list as many people as you can think of. Do you want me to write, or do you want to do the writing? First, think of people in your household—whom does that include? Now, going around the circle, what other family members would you include in your network? How about people from work or school? (Proceed around each segment of the circle.) Finally, list professional people or people from formal agencies whom you have contact with.
Look over your network. Are these the people you would consider part of your social network this past month? (Add or delete names as needed.)
Step two. Number the sections of the circle 1 through 7, as shown in the Area of Life section of the grid (exhibit 6-3). If there are more than 15 names on the circle, the client selects the top 15 people to enter on the social network grid. Transfer the 15 names and the numbers that correspond to the sections of the map to the social network grid. Names of people in the network also should be put on individual slips of paper for the client to use in preparing the network grid.
Exhibit 6-3. Social Network Grid Used in Conjunction With Network Map
| ID________ | Area of life | Concrete support | Emotional support | Information/ advice | Critical of client | Direction of help | Closeness | How often seen | How long known | |
|---|---|---|---|---|---|---|---|---|---|---|
| Respondent | 1. Household | 1. Hardly ever | 1. Hardly ever | 1. Hardly ever | 1. Hardly ever | 1. Goes both | 1. Never very | 0. Does not see | 1. < 1 yr. | |
| _______________ | 2. Other family | 2. Sometimes | 2. Sometimes | 2. Sometimes | 2. Sometimes | ways | close | 1. Few times/yr. | 2. 1–5 yrs. | |
| Name # | 3. Work/school | 3. Almost always | 3. Almost always | 3. Almost always | 3. Almost always | 2. You to them | 2. Sort of close | 2. Monthly | 3. > 5 yrs. | |
| 4. Organizations | 3. They to you | 3. Very close | 3. Weekly | |||||||
| 5. Other friends | 4. Daily/twice or more per week | |||||||||
| 6. Neighbors | ||||||||||
| 7. Formal services | ||||||||||
| 01 | ||||||||||
| 02 | ||||||||||
| 03 | ||||||||||
| 04 | ||||||||||
| 05 | ||||||||||
| 06 | ||||||||||
| 07 | ||||||||||
| 08 | ||||||||||
| 09 | ||||||||||
| 10 | ||||||||||
| 11 | ||||||||||
| 12 | ||||||||||
| 13 | ||||||||||
| 14 | ||||||||||
| 15 | ||||||||||
Step three. After the names from the social network map have been added to the leftmost column of the social network grid, ask the client to consider the nine categories in the column headings. The client uses the 15 slips of paper with the names from the social network map to respond, sorting the slips into groups corresponding to the numerical options that accompany each category in the grid. For example, when considering how critical of the client each individual in his or her life is, the client sorts the slips into piles representing those who (1) hardly ever, (2) sometimes, or (3) almost always criticize. The name of each person and the appropriate number for his or her level of support are then entered onto the network grid in each life area. The finished grid gives an overall picture of support in the client's social network.
Sample script. Now, I'd like to learn more about the people in your network. I've put their names on this network grid with a number for the area of life. Now I'm going to ask a few questions about the ways in which they help you.
The first three questions have to do with the types of support people give you. Who would be available to help you out in concrete ways? For example, who would give you a ride if you needed one or pitch in to help you with a big chore or look after your belongings for a while if you were away? Divide your cards into three piles: those people you can hardly ever rely on for concrete help, those you can rely on sometimes, and those you'd almost always rely on for this type of help.
Now, who would be available to give you emotional support? For example, who would comfort you if you were upset or listen to you talk about your feelings? Again, divide your cards into three piles. (Proceed through remainder of the questions.)
Clinical Application
Mapping a client's social network provides a visual and numerical depiction of the client's significant relationships. The following aspects of social functioning are highlighted:
- Network size
- Availability of support
- Criticism client faces
- Closeness
- Reciprocity
- Direction of help
- Stability
- Frequency of contact
*Source:Tracy and Whittaker 1990, pp. 463–466. Reprinted with permission from Families in Society (www.familiesinsociety.org), published by the Alliance for Children and Families.
Appendix 6-C. Resources for Family-Based Services
Publications and Videos
A helpful reference is Family Therapy: An Overview (Goldenberg and Goldenberg 1985). This book presents a comparison of six theoretical models of family therapy, including the psychodynamic, experiential/humanistic, structural, communication, and behavioral models. Meyers and colleagues (2003) offer an overview of community reinforcement and family therapy (CRAFT) that emphasizes the approach's empirical support. Using concerned family members and friends, CRAFT works to bring those who deny they have a substance use disorder into treatment.
American Outreach Association (AOA) (www.americanoutreach.org). AOA is a private, nonprofit organization that produces pamphlets to help families cope with alcohol and substance abuse. The pamphlets can be downloaded from AOA's Web site. Topics include strategies on confronting children who use substances, effective ways for parents to communicate with their children, and ways to help someone with alcohol and drug abuse problems.
Films for the Humanities and Sciences (www.films.com). This organization offers 150 educational films on substance abuse, covering topics such as treatment issues and the effects of addiction on family members and including a series on young adults and substance abuse.
Gerald T. Rogers Productions (www.gtrvideo.com). This company produces films and videos on substance abuse for many audiences, from first graders to families with members who abuse substances.
Hazelden Foundation (www.hazeldenbookplace.org). Hazelden Bookplace is an online resource center and marketplace for products and services from Hazelden Publishing & Educational Services and provides resources to help individuals, families, and communities prevent and recover from substance use and related disorders.
Johnson Institute (johnsoninstitute.org). This organization offers books, booklets, and videos that are distributed through the Hazelden Bookplace Web site. Some family-related videotapes available are Parenting Issues for Recovering Families, The Kid and Me: Parenting for Prevention, The Enabler, Intervention, and Intervention: How to Help Someone Who Doesn't Want Help.
National Families in Action (NFIA) (www.nationalfamilies.org). NFIA is a national drug education, prevention, and policy center with the mission of helping families prevent substance abuse among children by promoting science-based policies. NFIA offers books, pamphlets, and afterschool programs to keep young people substance free. NFIA has collaborated with other organizations on several projects, including Allied Systems Strengthening Families Project and the Drug-Free America Foundation.
NIMCO, Inc. (www.nimcoinc.com). This organization offers videos on alcohol, tobacco, and drug education and prevention topics. Videos cover such issues as drinking and driving, steroid use, substance abuse in the workplace, and the effects of substance abuse on the mind and body.
Pyramid Media (www.pyramidmedia.com). This company offers films and videos about substance abuse that are appropriate for training, educational groups, and individual and family viewing.
Substance Abuse and Mental Health Services Administration's National Clearinghouse for Alcohol and Drug Information (NCADI) (www.ncadi.samhsa.gov). NCADI is a national resource center funded by the Federal Government that offers a large inventory of publications and videos for treatment professionals, clients, families, and the general public, including Alcoholism Tends To Run in Families. This fact sheet presents important information about the influence of parental alcoholism on children and families. It considers evidence that links alcoholism to dysfunctional marital relationships, child abuse, depression, physical problems, and impaired school performances, among other undesirable effects.
Moyers on Addiction: Close to Home (www.pbs.org/wnet/closetohome). This is the online companion to the PBS show. It features real-life stories of struggles with addiction, information on treatment and prevention, and downloadable resources such as family guides, viewer's guides, teacher's guides, and health professional's guides to the PBS series.
Family Support Groups
Adult Children of Alcoholics (ACOA) (www.adultchildren.org). ACOA is a 12-Step, 12-Tradition program that offers support for grown children of parents with alcohol or drug addiction.
Al-Anon family groups (www.al-anon.org). Al-Anon is a fellowship of relatives and friends of people who have alcohol problems who share their experiences, strengths, and hopes. Members believe that alcoholism is a family illness and that changed attitudes can aid recovery. The program is based on the 12 Steps and 12 Traditions of Alcoholics Anonymous.
Families Anonymous (FA) (www.familiesanonymous.org). FA is a 12-Step, mutual-help, recovery support group for relatives and friends of those who have alcohol, drug, or behavioral problems. FA pamphlets, booklets, newsletters, and daily inspirational thought book are written by the members.
Nar-Anon family groups (www.naranon.com). Similar to Al-Anon, Nar-Anon is a fellowship of relatives and friends of people who abuse substances and offers a constructive program for members to achieve peace of mind and to gain hope for the future. Contact information is available in local telephone directories.
National Asian Pacific American Families Against Substance Abuse (www.napafasa.org). This nonprofit organization is dedicated to addressing the alcohol, tobacco, and drug issues of Asian and Pacific Islander (API) populations in the continental United States, Hawaii, and the six Pacific Island jurisdictions, as well as elsewhere. Its nationwide network consists of approximately 200 API and human service organizations, and its Web site lists resources, services for public and professional audiences, and current activities.
- Chapter 6. Family-Based Services - Substance Abuse: Clinical Issues in Intensive...Chapter 6. Family-Based Services - Substance Abuse: Clinical Issues in Intensive Outpatient Treatment
Your browsing activity is empty.
Activity recording is turned off.
See more...